

In psoriatic arthritis patients, the primary efficacy end point at Week 12 in RAPID-PsA was ACR20, with 58% of CIMZIA 200 mg Q2W patients achieving ACR20 at Week 12 vs. 24% of placebo patients.1,2*
*RS-NRI: randomized set non-responder imputation.
ACR20: American College of Rheumatology criteria for 20% response; PsA: psoriatic arthritis; Q2W: every 2 weeks.
Oliver’s tried various treatments as a long-time psoriasis patient. Recently, his dermatologist recommended CIMZIA for his newly diagnosed psoriatic arthritis. With CIMZIA, Oliver experienced results he could see and feel.

Rapid-PsA
ACR20/50/70 response rates in CIMZIA 200 mg Q2W patients1-3*†
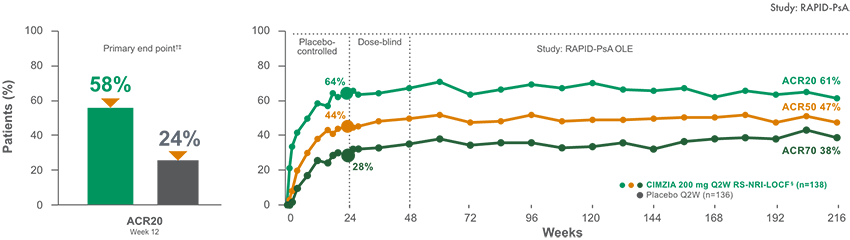
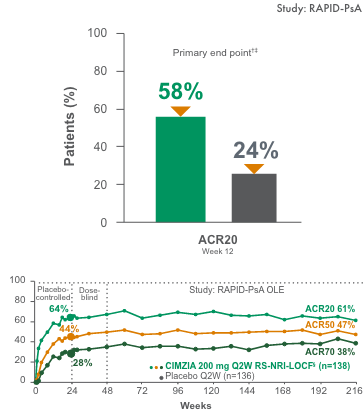
CIMZIA helped some patients achieve an ACR20 response as early as 1 to 2 weeks.1,2II
- Placebo [n=136] rates at Week 24—ACR20: 24%; ACR50: 13%; ACR70: 4%1,2
- Line graph to Week 216 represents patients who were randomized initially to CIMZIA 200 mg Q2W
- ACR response criteria assess changes in swollen and tender joints, pain, functional ability, patient and physician global assessment, and acute-phase reactant. ACR20/50/70 relates to 20%, 50%, and 70% response improvement
- Limitations OLE data: Potential bias due to open-label treatment and no long-term placebo comparator for ACR responder rates beyond Week 24
- RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and OLE through Week 2162
IMPORTANT SAFETY INFORMATION
Patients treated with CIMZIA are at an increased risk for developing serious infections involving various organ systems and sites that may lead to hospitalization or death. Patients greater than 65 years of age, patients with co-morbid conditions, and/or patients taking concomitant immunosuppressants (e.g. corticosteroids or methotrexate) may be at a greater risk of infection.
| * | The same patients may not have responded at each timepoint.1-3 |
| † | RS-NRI: Randomized set non-responder imputation. |
| ‡ | P<0.001 vs. placebo.1-3 |
| § | RS-NRI-LOCF: Randomized set. Non-responder imputation LOCF. |
| || | 58% of CIMZIA patients at 12 weeks vs. 24% of placebo patients; 22% and 33% of CIMZIA patients at 1-2 weeks vs. 7% and 12% of placebo patients, respectively.1,2,4 |
ACR: American College of Rheumatology; LOCF: last observation carried forward; OLE: open-label extension; PsA: psoriatic arthritis; Q2W: every 2 weeks.
- The radiographic primary end point was mean change from baseline in mTSS at Week 24 (‑0.02 with CIMZIA 200 mg Q2W [n=138] vs. 0.18 with placebo [n=136]; P<0.05)1,2†
- Patients treated with CIMZIA 400 mg Q4W did not demonstrate greater inhibition of radiographic progression compared with placebo-treated patients at Week 24
- Limitations of OLE: Weeks 48 through 216 were an OLE phase of the study. As with any long-term, uncontrolled OLE, there were several limitations with this portion of the study. Limitations of OLE data include potential bias due to open-label treatment, lack of long-term control beyond Week 24, and potential enrichment of population with responders
IMPORTANT SAFETY INFORMATION
Cases of lymphoma and other malignancies have been observed among patients receiving TNF blockers, including children, adolescents, and young adults. Acute and chronic cases of leukemia have also been reported. Postmarketing cases of hepatosplenic T-cell lymphoma (HSTCL), a rare type of T-cell lymphoma that has a very aggressive disease course and is usually fatal, have been reported in patients treated with TNF blockers, including CIMZIA. Melanoma and Merkel cell carcinoma have been reported in patients treated with TNF-antagonists, including CIMZIA. Periodic skin examinations are recommended for all patients, particularly those with risk factors for skin cancer.
| * | “No progression” was defined as a change from baseline in mTSS of ≤0.5. When “no progression” was defined as a change from baseline in mTSS of ≤0, 63.3% of x-rayed patients experienced no progression. Results are from observed case analysis.3 |
| † | Randomized set. For placebo patients who escaped early to CIMZIA, the Week 24 values were linearly extrapolated; ANCOVA model. For patients with two radiographs, but a missing Week 24 or baseline film, linear extrapolation was performed in all approaches. Results are from observed case analysis.3 |
mTSS: modified Total Sharp Score; OLE: open-label extension; Q2W: every 2 weeks; Q4W: every 4 weeks.
Safety profile for PsA in the RAPID-PsA study1,2
Incidence of TEAEs through Week 241,2
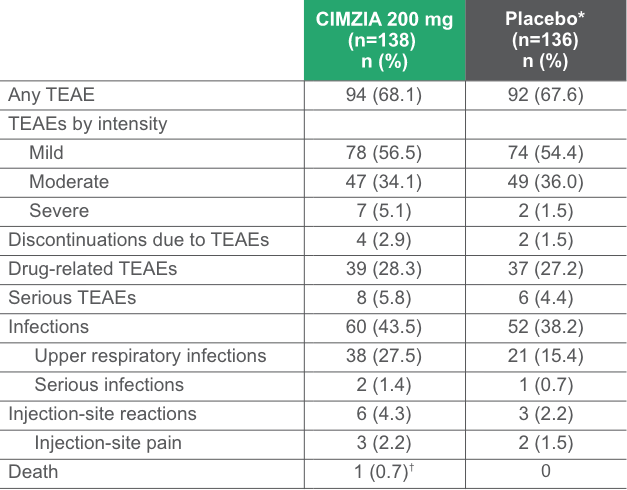
*Placebo escape at Week 16; data not adjusted for exposure.2
†Myocardial infarction. Considered unrelated to study medication by investigators.2
TEAEs with an incidence of >3% of patients (CIMZIA 200 mg) through Week 241,2
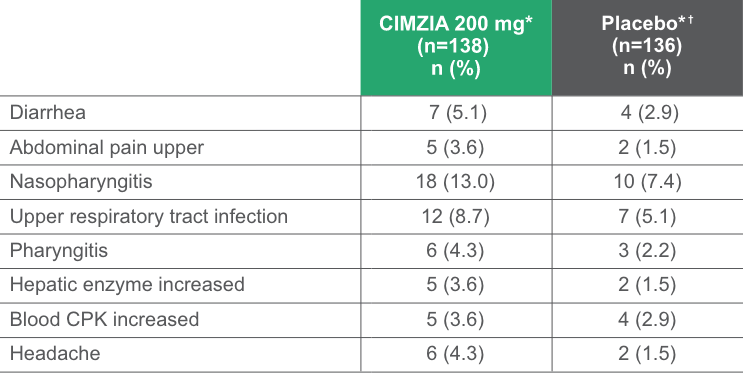
- Most AEs were mild to moderate in severity
*Not adjusted for exposure.
†Placebo escape at Week 16.2
AE: adverse event; CPK: creatine phosphokinase; PsA: psoriatic arthritis; TEAE: treatment-emergent adverse event.
IMPORTANT SAFETY INFORMATION
Cases of worsening congestive heart failure (CHF) and new onset CHF have been reported with TNF blockers.
No new safety signals were identified through Week 216.1,2
Total resolution of dactylitis over 216 weeks3,4

Not an actual patient.
Post hoc analysis from 4-year OLE of RAPID-PsA3,4

Post hoc analysis: Total resolution defined as having at least one (1) digit affected and with a difference in circumference ≥10% compared with the opposite digit (LDI >0), achieving complete clearance (LDI=0).
- 34% of CIMZIA patients and 33% of placebo patients had dactylitis at baseline4
- Prespecified secondary end point was “Change from baseline in the LDI at Weeks 12 and 24 (other timepoints were exploratory)”
- Limitations of OLE data: Potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
- This subgroup analysis is a post hoc analysis. The RAPID-PsA study was not powered for this subgroup analysis, nor was the analysis error-controlled. Therefore, these results should be interpreted with caution, and the data observed in this subgroup cannot be regarded as statistically significant
IMPORTANT SAFETY INFORMATION
Anaphylaxis or serious allergic reactions may occur. Some of these reactions occurred after the first administration of CIMZIA. Hypersensitivity reactions have been reported rarely following CIMZIA administration. The needle shield inside the removable cap of the CIMZIA prefilled syringe contains a derivative of natural rubber latex which may cause an allergic reaction in individuals sensitive to latex.
CZP: certolizumab pegol; LDI: Leeds Dactylitis Index; LOCF: last observation carried forward; OC: observed case; OLE: open-label extension; PsA: psoriatic arthritis; Q2W: every 2 weeks; Q4W: every 4 weeks.
Total resolution of enthesitis in combined CZP dose (OC and LOCF)3,4

Not an actual patient.
Post hoc analysis from 4-year OLE of RAPID-PsA4
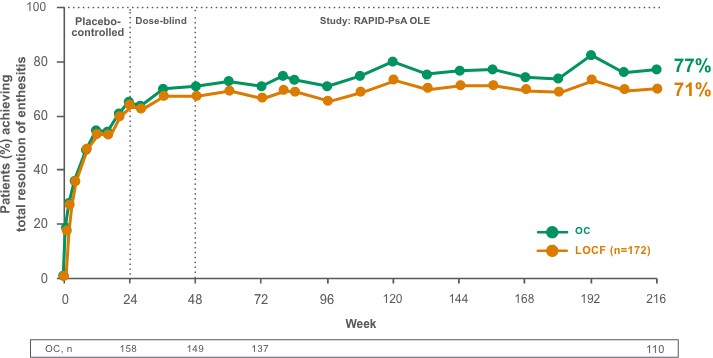
Post hoc analysis: Total resolution of enthesitis defined as the percentage (%) of patients with baseline involvement (LEI>0) achieving complete clearance (LEI=0).
- 64% of CIMZIA patients and 67% of placebo patients had enthesitis at baseline2
- Prespecified secondary end point was “Change from baseline in the LEI at Weeks 12 and 24 (other timepoints were exploratory)”
- Limitations of OLE data: Potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
- This subgroup analysis is a post hoc analysis. The RAPID-PsA study was not powered for this subgroup analysis, nor was the analysis error-controlled. Therefore, these results should be interpreted with caution, and the data observed in this subgroup cannot be regarded as statistically significant
- CIMZIA combined dose included patients receiving CIMZIA 200 mg Q2W and patients receiving CIMZIA 400 mg Q4W. All CIMZIA patients received a loading dose of 400 mg at Weeks 0, 2, and 4
IMPORTANT SAFETY INFORMATION
Use of TNF blockers, including CIMZIA, has been associated with reactivation of hepatitis B virus in patients who are chronic carriers of the virus. In some instances, HBV reactivation occurring in conjunction with TNF-blocker therapy has been fatal.
CZP: certolizumab pegol; LEI: Leeds Enthesitis Index; LOCF: last observation carried forward; OC: observed case; OLE: open-label extension; PsA: psoriatic arthritis; Q2W: every 2 weeks; Q4W: every 4 weeks.
Total resolution of nail psoriasis in the combined CIMZIA dose group (OC and LOCF)3,4

Not an actual patient.
Post hoc analysis from 4-year OLE of RAPID-PsA3,4
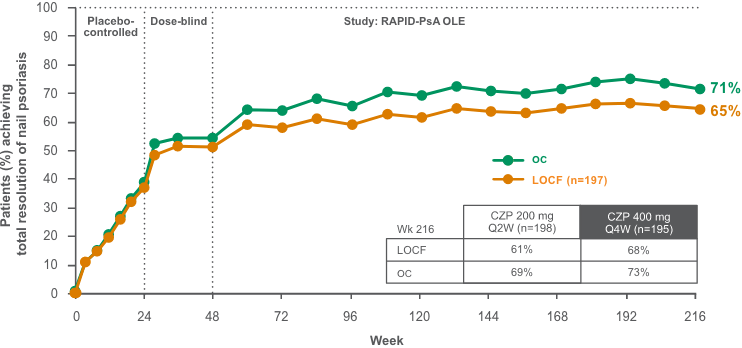
Post hoc analysis: Total resolution of nail psoriasis defined as the percentage (%) of patients with baseline involvement (mNAPSI >0) achieving complete clearance (mNAPSI=0).3,4
- 72% of CIMZIA patients and 76% of placebo patients had nail psoriasis at baseline3,4
- mNAPSI in patients with nail disease at baseline (assessing only the most affected nail at baseline) was a specified other efficacy outcome in the RAPID-PsA study
- Limitations of OLE data: Potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
- This subgroup analysis is a post hoc analysis (not a primary or secondary outcome)
- CIMZIA combined dose included patients receiving CIMZIA 200 mg Q2W and patients receiving CIMZIA 400 mg Q4W. All CIMZIA patients received a loading dose of 400 mg at Weeks 0, 2, and 4
IMPORTANT SAFETY INFORMATION
Treatment with TNF blockers, including CIMZIA, may rarely result in new onset or exacerbation of clinical symptoms and/or radiographic evidence of central or peripheral nervous system demyelinating disease, as well as the development of a lupus-like syndrome.
CZP: certolizumab pegol; LOCF: last observation carried forward; mNAPSI: Modified Nail Psoriasis Severity Index; OC: observed case; OLE: open-label extension; PsA: psoriatic arthritis; Q2W: every 2 weeks; Q4W: every 4 weeks.
Change from baseline in patient’s global assessment of arthritis pain through Year 43,4*†
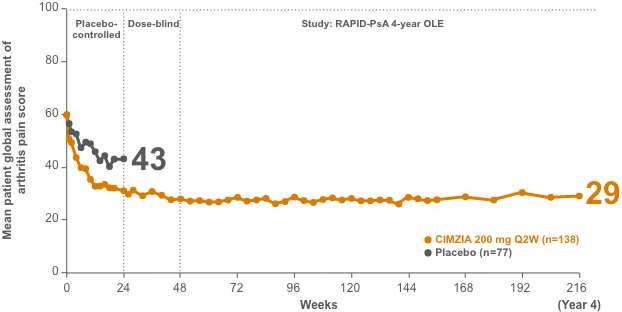
- Baseline pain score was 60 (VAS: 0=no pain and 100=most severe pain) for both the placebo arm and the CIMZIA 200 mg Q2W arm3,4
- Data were imputed using NRI for missing categorical data
- Limitations of OLE data: Potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
IMPORTANT SAFETY INFORMATION
Rare reports of blood dyscrasias have been reported with CIMZIA; patients should be advised to seek medical attention if they develop.
*Pain assessment is a part of the ACR score. Pain assessment is done by the patient; hence, individual assessment/score may vary from patient-to-patient.
†Patient assessment of arthritis pain, VAS: 0=no pain, 100=most severe pain.
ACR: American College of Rheumatology; NRI: non-responder imputation; OLE: open-label extension; PsA: psoriatic arthritis: Q2W: every 2 weeks; VAS: visual analog scale.
RAPID-PsA study: Mean improvement from baseline in physical function (HAQ-DI)1,2,4
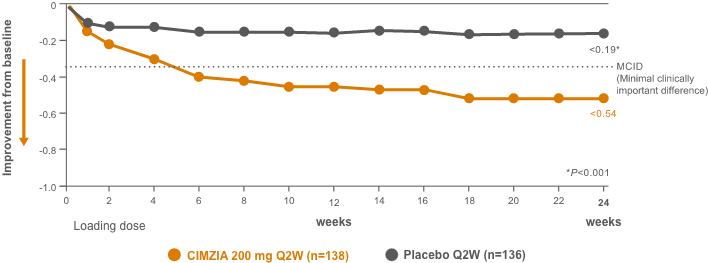
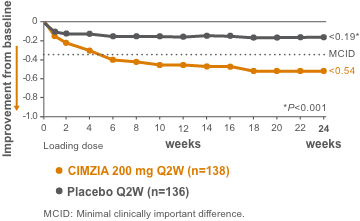
CIMZIA significantly improved the signs and symptoms of disease for PsA patients.1,2,4
- Change from baseline in the HAQ-DI score was a prespecified secondary end point at Week 24
- Baseline HAQ-DI score was 1.30 for the placebo arm and 1.33 for the CIMZIA 200 mg Q2W arm
- MCID was defined as a reduction in HAQ-DI from baseline of ≥0.3
- Graph data represent randomized set LOCF for patients withdrawn for any reason, missing Week 24 measurement, or placebo patients who used escape treatment
IMPORTANT SAFETY INFORMATION
Patients on CIMZIA should not receive live or live-attenuated vaccines.
HAQ-DI: Health Assessment Questionnaire-Disability Index; LOCF: last observation carried forward; PsA: psoriatic arthritis; Q2W: every 2 weeks.
ACR20 responder rates at 4 years in RAPID-PsA (NRI)3*
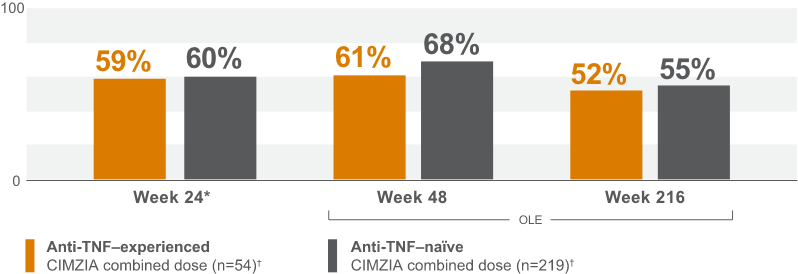
Limitations of OLE data: ACR responder rates did not have a long-term placebo comparator beyond Week 24. 20% of patients had prior anti-TNF exposure, primary non-responders excluded.3
IMPORTANT SAFETY INFORMATION
Concurrent administration of CIMZIA with certain biological DMARDs, including anakinra, abatacept and rituximab, is not recommended due to an increased risk of serious infections.
*Randomized set. Non-responder imputation.
†CIMZIA combined dose included patients receiving CIMZIA 200 mg Q2W and patients receiving CIMZIA 400 mg Q4W.
ACR: American College of Rheumatology; NRI: non-responder imputation; OLE: open-label extension; PsA: psoriatic arthritis; Q2W: every 2 weeks; Q4W: every 4 weeks; TNF: tumor necrosis factor.
RAPID-PsA (PsA001) study design2,3
RAPID-PsA (PsA001) study design2,3
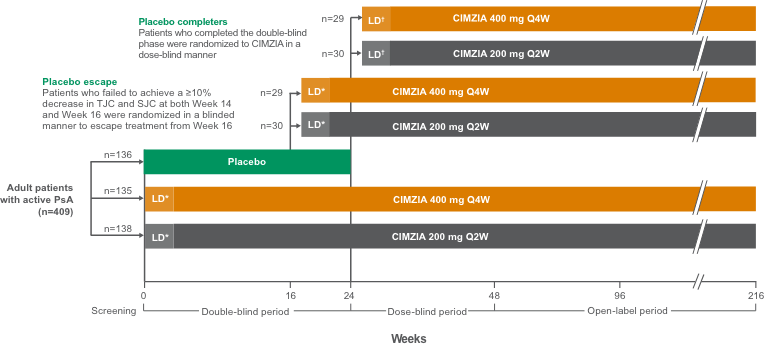
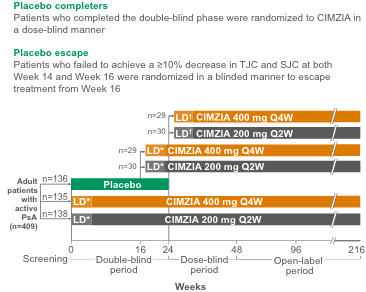
*Loading dose of CIMZIA 400 mg at Weeks 0, 2, and 4 or Weeks 16, 18, and 20.
†Loading dose of 400 mg at Weeks 24, 26, and 28.
LD: loading dose; PsA: psoriatic arthritis; SJC: swollen joint count; TJC: tender joint count; Q2W: every 2 weeks; Q4W: every 4 weeks.
CIMplicity supports your patients every step of the way
Learn about same-day benefits verification, PA, and how commercially insured, eligible patients whose coverage is delayed or denied can start treatment right away, at no cost.*†

Find on-demand education at DermDiscovery
Take a closer look at the only PEGylated Fc-Free anti-TNF1
See the CIMZIA mechanism of action.
| * | Requires PA to be submitted. |
| † | Eligible patients with a valid prescription for CIMZIA can receive treatment with the CIMZIA Prefilled Syringe at no cost for up to 24 months or until the patient’s coverage is approved, whichever comes first. Program is not available to patients whose medications are reimbursed in whole or in part by Medicare, Medicaid, TRICARE, or any other federal or state program or where otherwise prohibited by law. Patients may be asked to reverify insurance coverage status during the course of the program. No purchase necessary. Program is not health insurance, nor is participation a guarantee of insurance coverage. Limitations may apply. For initial enrollment into the Program the patient must be required by his/her commercial insurer to submit a prior authorization, or insurance coverage for the CIMZIA Prefilled Syringe must be unavailable. To maintain eligibility in the Program, the following are required: (1) a submitted prior authorization is denied or coverage remains unavailable for the patient; and (2) the prescriber must submit an appeal within 45 days of the first two denials and quarterly thereafter. UCB reserves the right to rescind, revoke, or amend this Program without notice. |
Fc: fragment crystallizable; PA: prior authorization; PEG: polyethylene glycol; TNF: tumor necrosis factor.