

CIMZIA delivered sustained joint improvement over 4 years
ACR20/50/70 response rates in CIMZIA
200 mg Q2W patients (n=138)1-3† ACR20/50/70 response rates in CIMZIA 200 mg Q2W patients (n=138)1-3*†
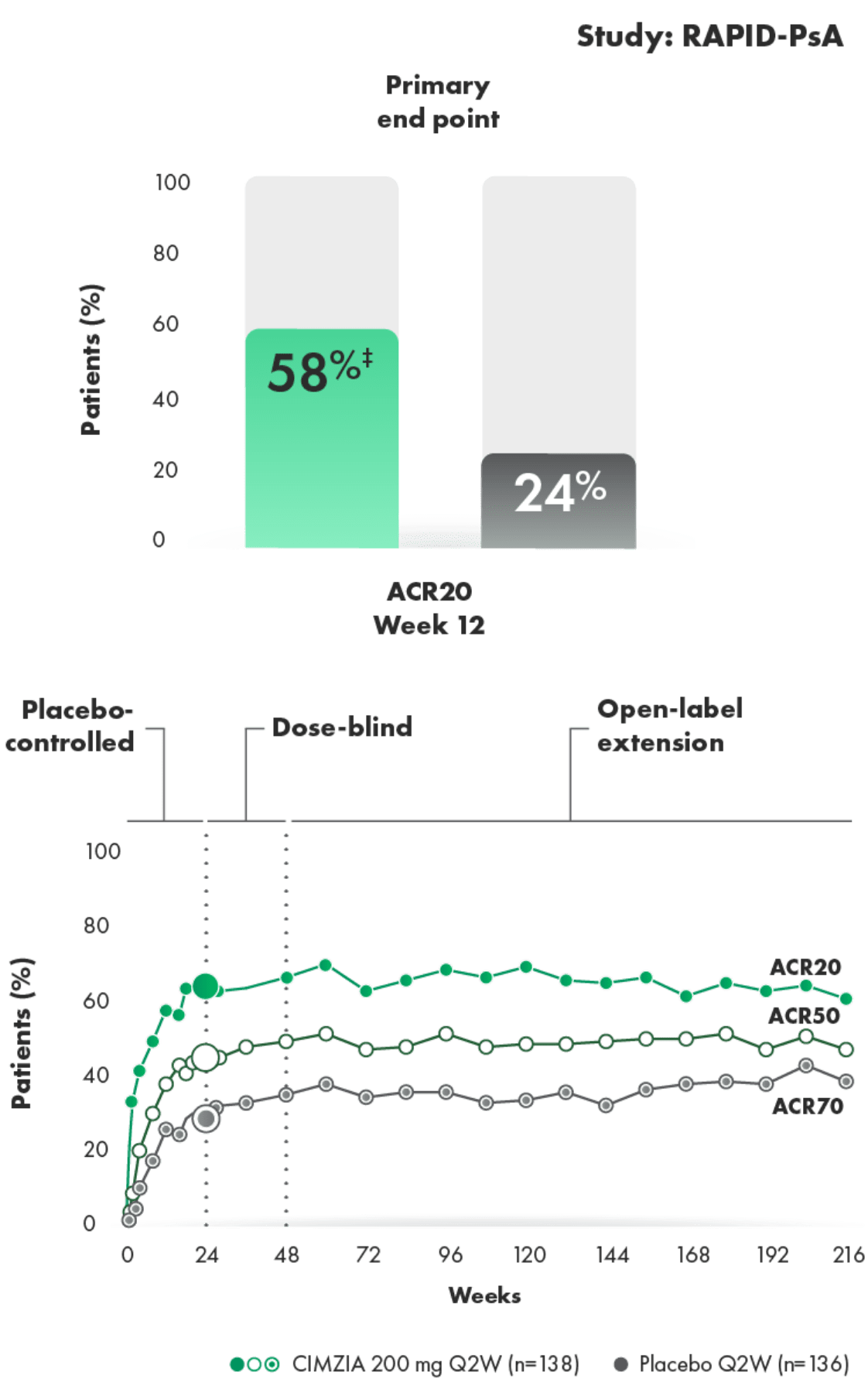
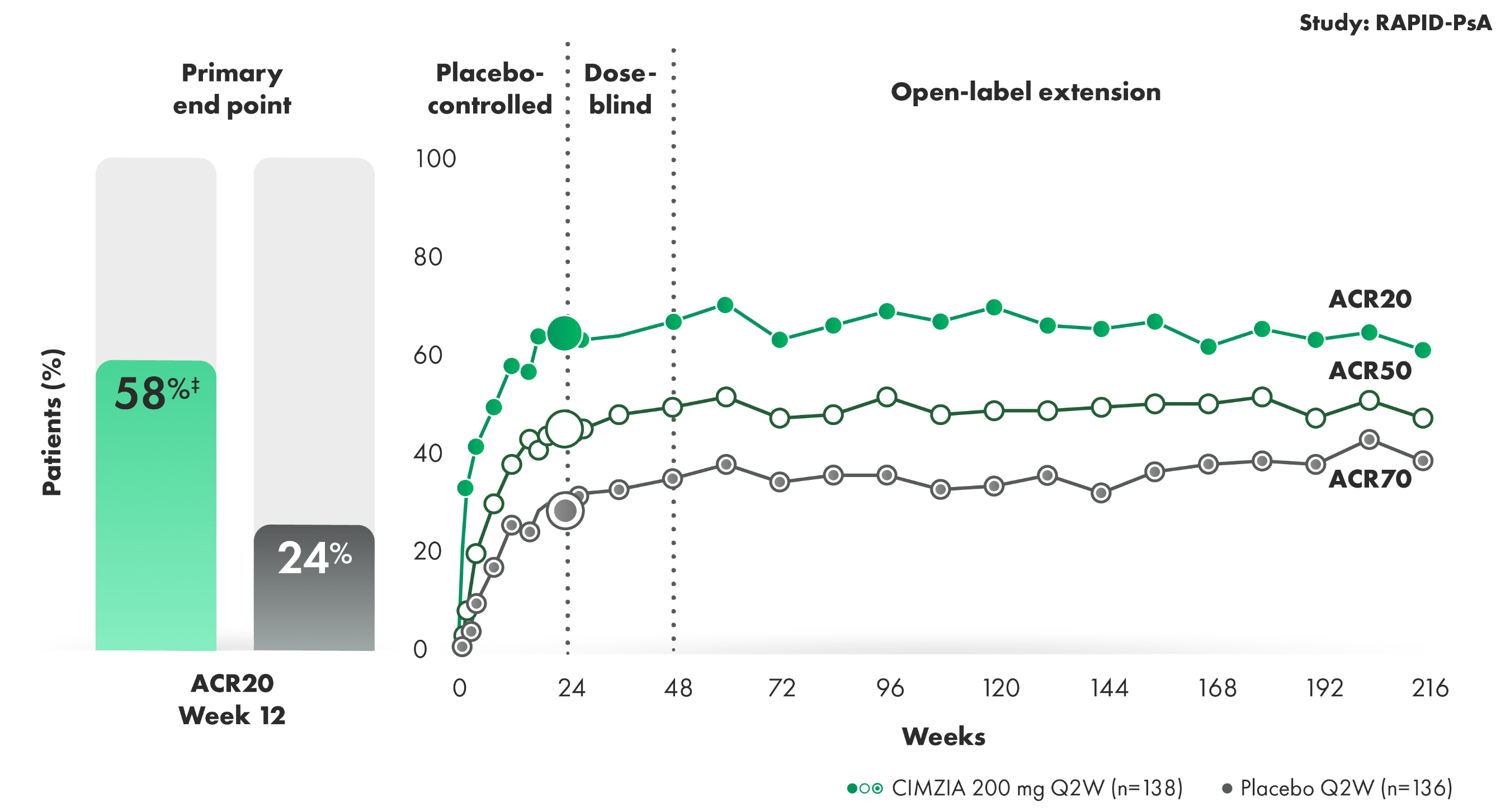
SOME CIMZIA PATIENTS ACHIEVED AN ACR20 RESPONSE AS EARLY AS 1 TO 2 WEEKS1,2
- Placebo (n=136) rates at Week 24—ACR20: 24%; ACR50: 13%; ACR70: 4%1,2
- ACR response criteria assess changes in swollen and tender joints, pain, functional ability, patient and physician global assessment, and acute-phase reactant
- Limitation of OLE data: Potential bias due to open-label treatment and no long-term placebo comparator for ACR responder rates beyond Week 24
- Line graph to Week 216 represents patients who were randomized initially to CIMZIA 200 mg Q2W
*The same patients may not have responded at each time point.1-3
†RS-NRI: randomized set nonresponder imputation.
‡P<0.001 vs. placebo.1-3
RAPID-PsA2
RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and open-label through Week 216. In this study, 409 patients who had failed ≥1 DMARD (non-biologic or biologic) were randomized (1:1:1) to CIMZIA 200 mg Q2W (n=138), CIMZIA 400 mg Q4W (n=135), or placebo (n=136). Patients were stratified by prior TNFi exposure; primary nonresponders were excluded.
CIMZIA inhibited progression of structural damage
Mean change in mTSS at Week 241,2§||
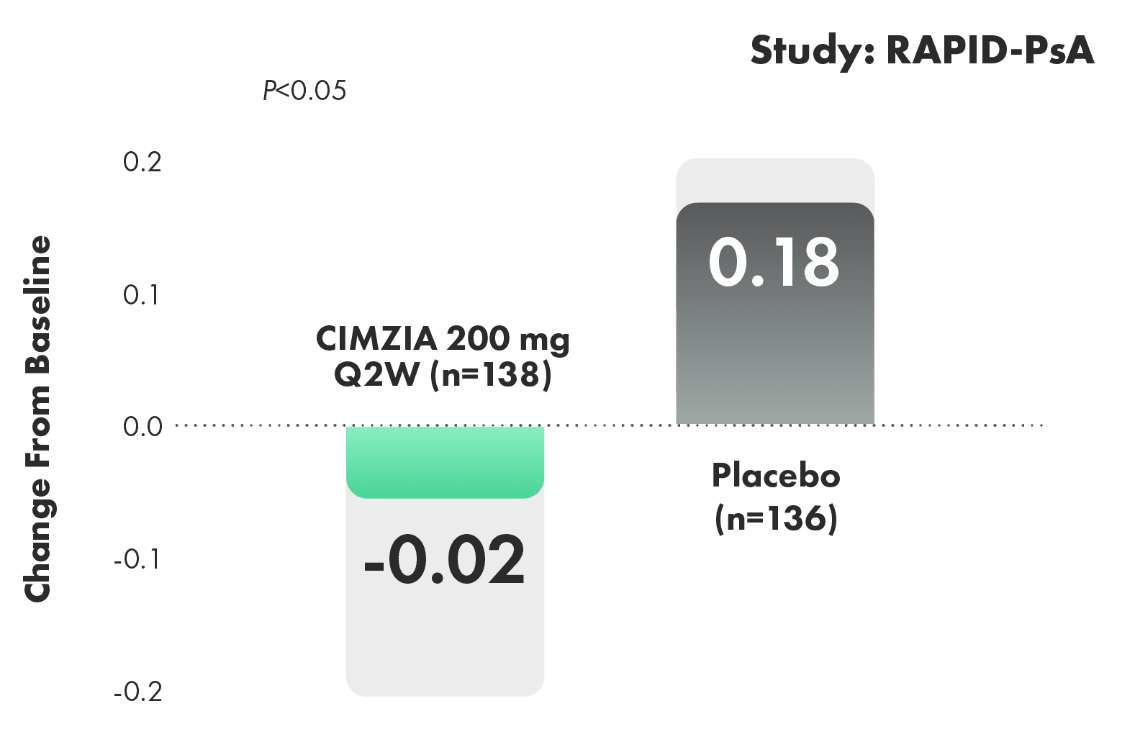
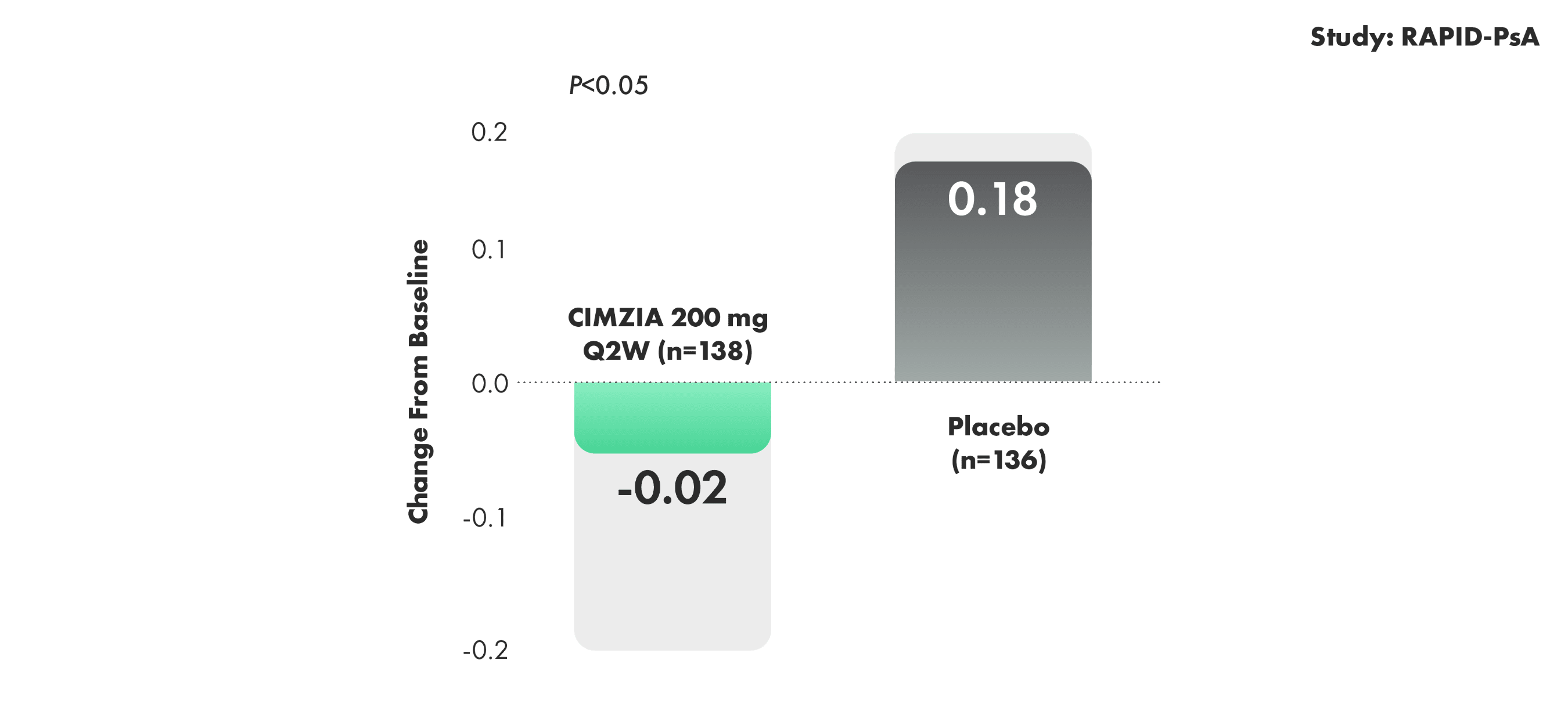
OF THOSE RECEIVING CIMZIA 200 mg Q2W (n=98), 8 OF 10
X-RAYED PATIENTS EXPERIENCED NO RADIOGRAPHIC PROGRESSION OVER 4 YEARS3¶OF THOSE RECEIVING CIMZIA 200 mg Q2W (n=98), 8 OF 10
X-RAYED PATIENTS EXPERIENCED NO RADIOGRAPHIC PROGRESSION OVER 4 YEARS3¶
X-rayed patients receiving CIMZIA 200 mg Q2W were analyzed using observed case analysis. Radiographic data do not have long-term placebo comparison beyond 24 weeks.
Patients treated with CIMZIA 400 mg Q4W did not demonstrate greater inhibition of radiographic progression compared with placebo-treated patients at Week 24.
- Limitations of OLE data include potential bias due to open-label treatment, lack of long-term placebo control beyond Week 24, and potential enrichment of population with responders
§Randomized set; for placebo patients who escaped early to CIMZIA, the Week 24 values were linearly extrapolated; ANCOVA model.3
||For placebo patients who escaped early to CIMZIA, the Week 24 values were linearly extrapolated. The P value of CIMZIA vs. placebo is based on ANCOVA. For patients with 2 radiographs, but a missing Week 24 or baseline film, linear extrapolation was performed in all approaches.
¶“No progression” was defined as a change from baseline in mTSS of ≤0.5. When “no progression” was defined as a change from baseline in mTSS of ≤0, 63.3% of X-rayed patients experienced no progression.4
ACR, American College of Rheumatology; ANCOVA, analysis of covariance; DMARD, disease-modifying antirheumatic drug; mTSS, modified Total Sharp Score; OLE, open-label extension; PsA, psoriatic arthritis; Q2W, every 2 weeks; Q4W, every 4 weeks; TNFi, tumor necrosis factor inhibitor.
CIMZIA delivered skin improvements over 4 years
PASI 75/90/100 response rates in a subpopulation of CIMZIA 200 mg Q2W patients with PsA (n=90)1,2*†
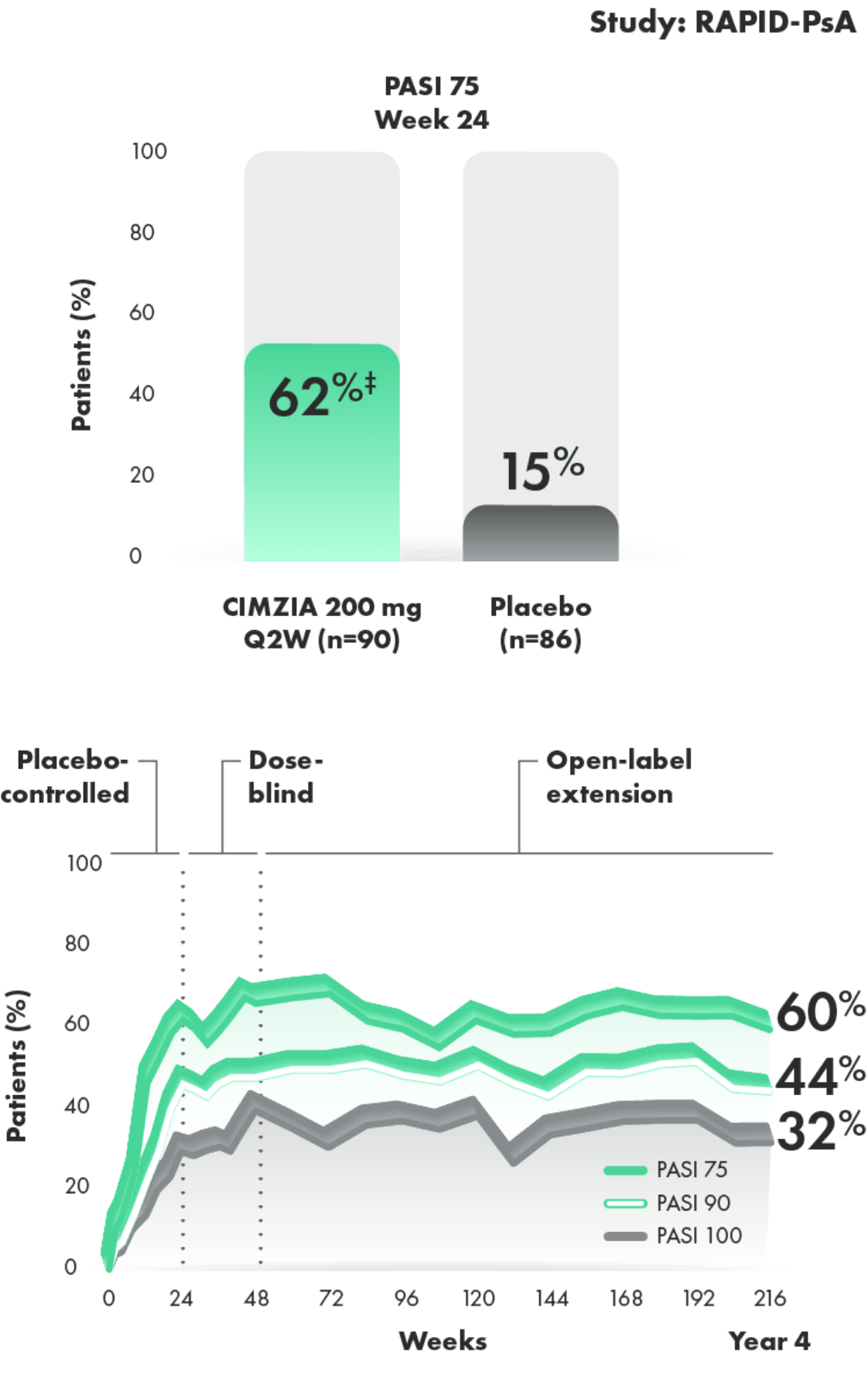
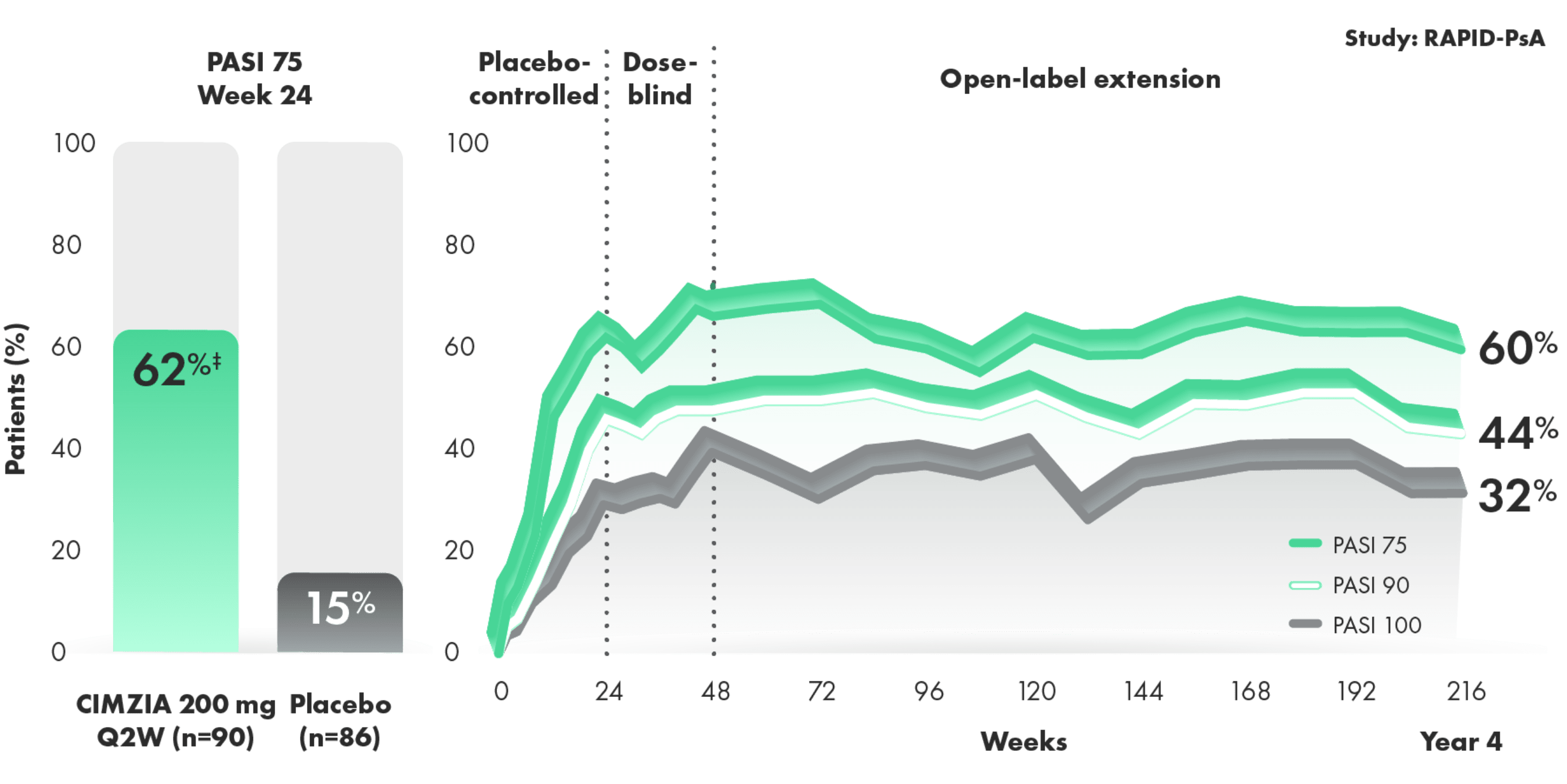
- Placebo rates at Week 24—PASI 90: 6%; PASI 100: 2%2
- Baseline psoriatic skin involvement ≥3% of body surface area (62% overall) and median PASI at baseline was 7.1 for placebo and 7.0 for CIMZIA2
- Limitations of OLE data include potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
*RS-NRI: randomized set nonresponder imputation.
†PASI 75 response rate at Week 24 in patients with baseline psoriatic skin involvement ≥3% body surface area was a prespecified secondary end point for the combined dose CIMZIA group.
‡Nominal P value.
RAPID-PsA2
RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and open-label through Week 216. In this study, 409 patients who had failed ≥1 DMARD (non-biologic or biologic) were randomized (1:1:1) to CIMZIA 200 mg Q2W (n=138), CIMZIA 400 mg Q4W (n=135), or placebo (n=136). Patients were stratified by prior TNFi exposure; primary nonresponders were excluded.
DMARD, disease-modifying antirheumatic drug; OLE, open-label extension; PASI, Psoriasis Area and Severity Index; PsA, psoriatic arthritis; Q2W, every 2 weeks; Q4W, every 4 weeks; TNFi, tumor necrosis factor inhibitor.
Total resolution of enthesitis over 4 years (post hoc analysis of combined doses from 4-year OLE of RAPID-PsA)3,4
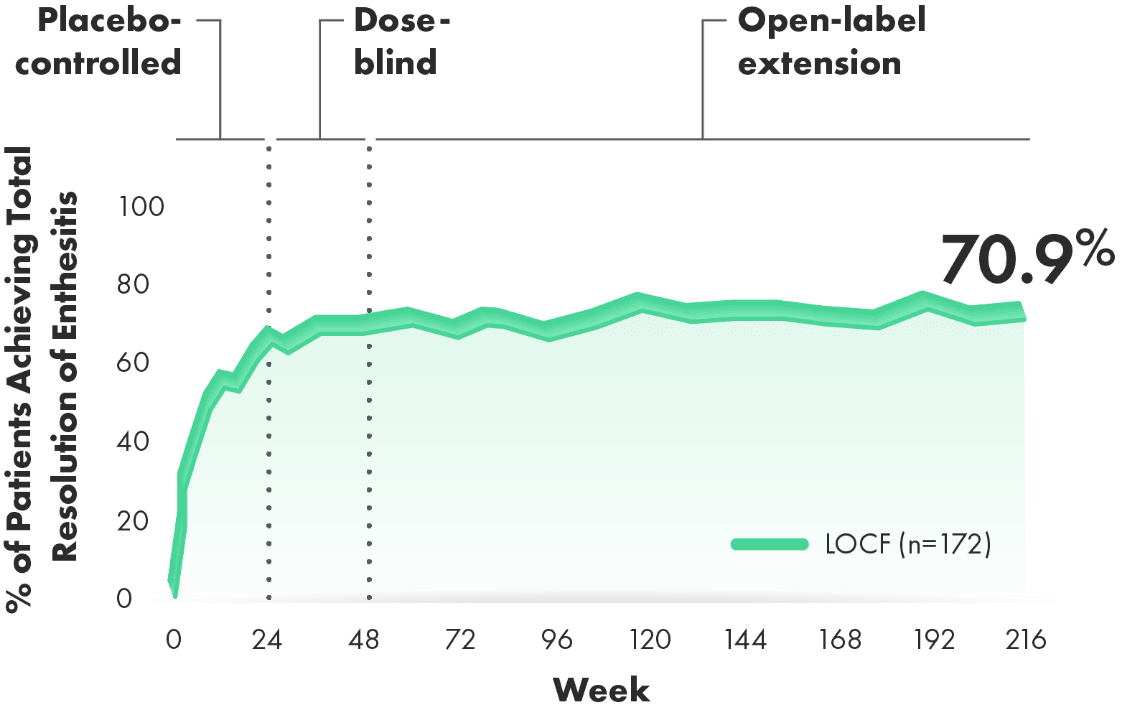
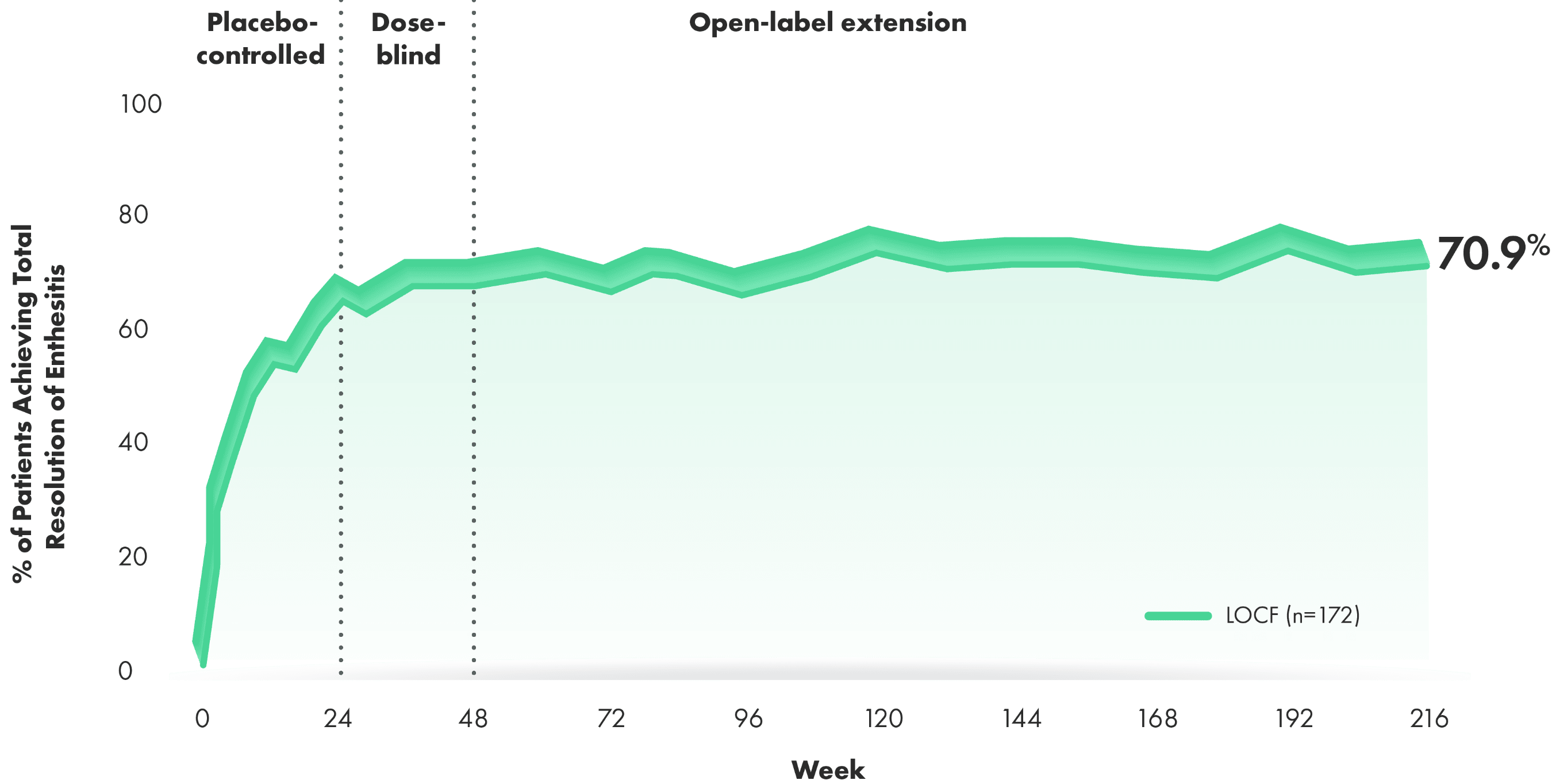
~7 OF EVERY 10 PATIENTS WITH BASELINE INVOLVEMENT ACHIEVED TOTAL RESOLUTION OF ENTHESITIS OVER 4 YEARS3,4
Post hoc analysis: Total resolution of enthesitis defined as reduction to LEI=0 from baseline LEI>0.
- 63% of CIMZIA patients and 67% of placebo patients had enthesitis at baseline2
- Prespecified secondary end point was change from baseline in LEI at Weeks 12 and 24 (other time points were exploratory)
- Limitations of OLE data include potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
- This subgroup analysis is a post hoc analysis. The RAPID-PsA study was not powered for this subgroup analysis, nor was the analysis error controlled. Therefore, these results should be interpreted with caution, and the data observed in this subgroup cannot be regarded as statistically significant
Total resolution of dactylitis over 4 years (RS, LOCF) (post hoc analysis from 4‑year OLE of RAPID-PsA)3,4
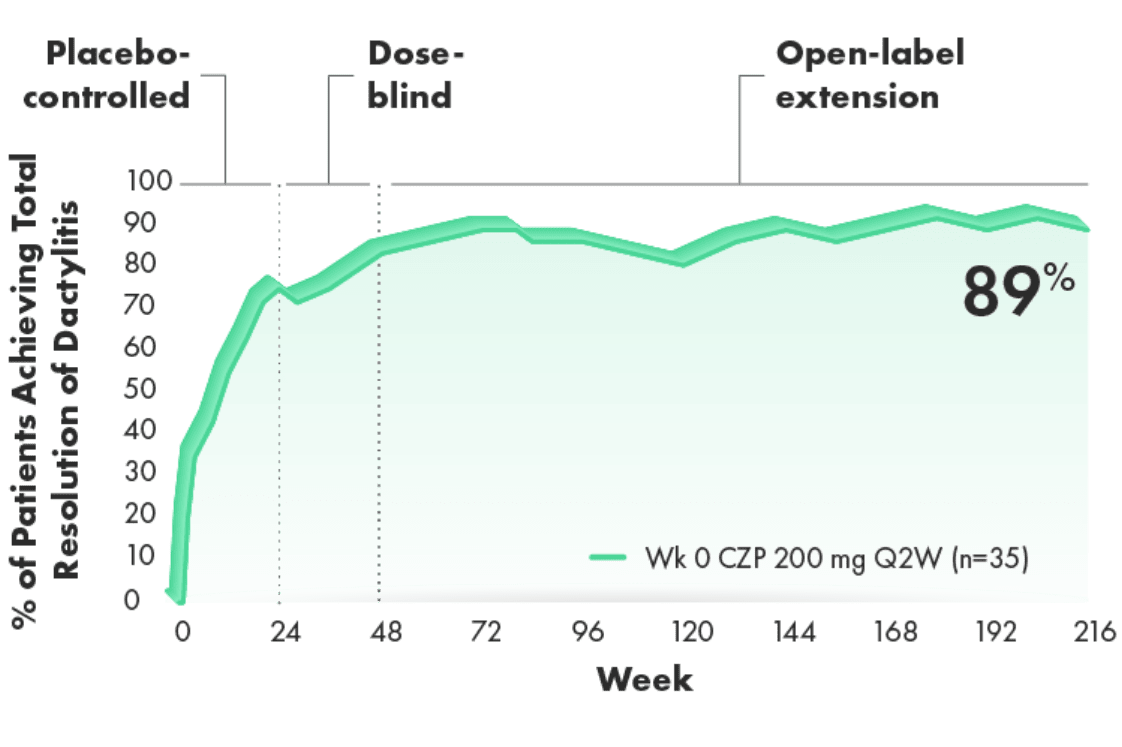
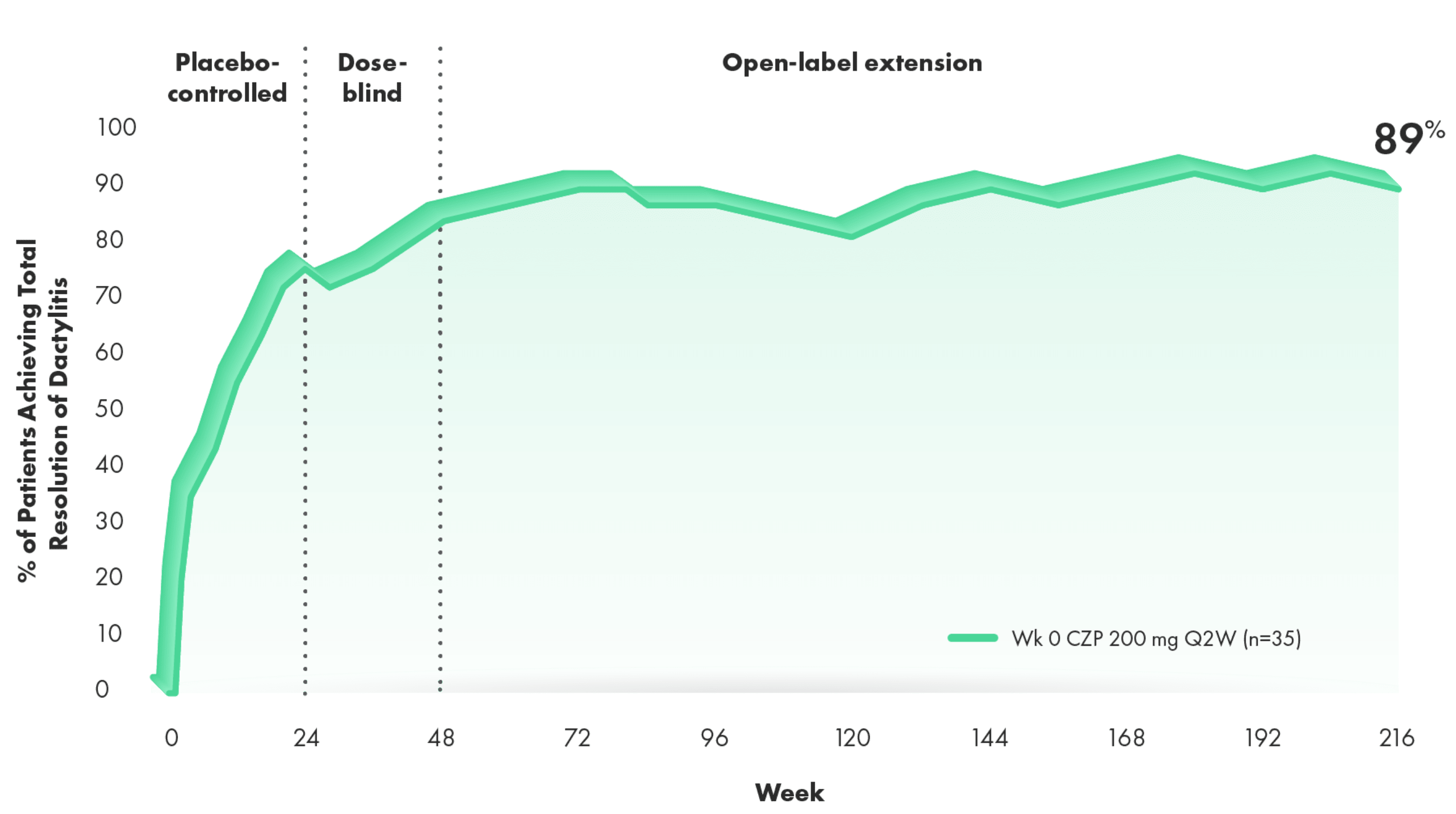
>8 OF EVERY 10 PATIENTS WITH BASELINE INVOLVEMENT ACHIEVED TOTAL RESOLUTION OF DACTYLITIS3,4
Post hoc analysis, RS, LOCF (n=35 patients with LDI >0 at baseline): Total resolution defined as LDI=0 in patients who at baseline had at least 1 digit affected and with a difference in circumference ≥10% compared with the opposite digit LDI>0.
- 34% of CIMZIA patients and 33% of placebo patients had dactylitis at baseline4
- Prespecified secondary end point was change from baseline in LDI at Weeks 12 and 24 (other time points were exploratory)
- Limitations of OLE data include potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
- This subgroup analysis is a post hoc analysis of the CZP 200 mg study arm of RAPID-PsA. The RAPID-PsA study was not powered for this subgroup analysis, nor was the analysis error controlled. Therefore, these results should be interpreted with caution, and the data observed in this subgroup cannot be regarded as statistically significant
Total resolution of nail psoriasis in the most severe nail of the hand over 4 years (LOCF)
(post hoc analysis from 4-year OLE of RAPID-PsA)3,4
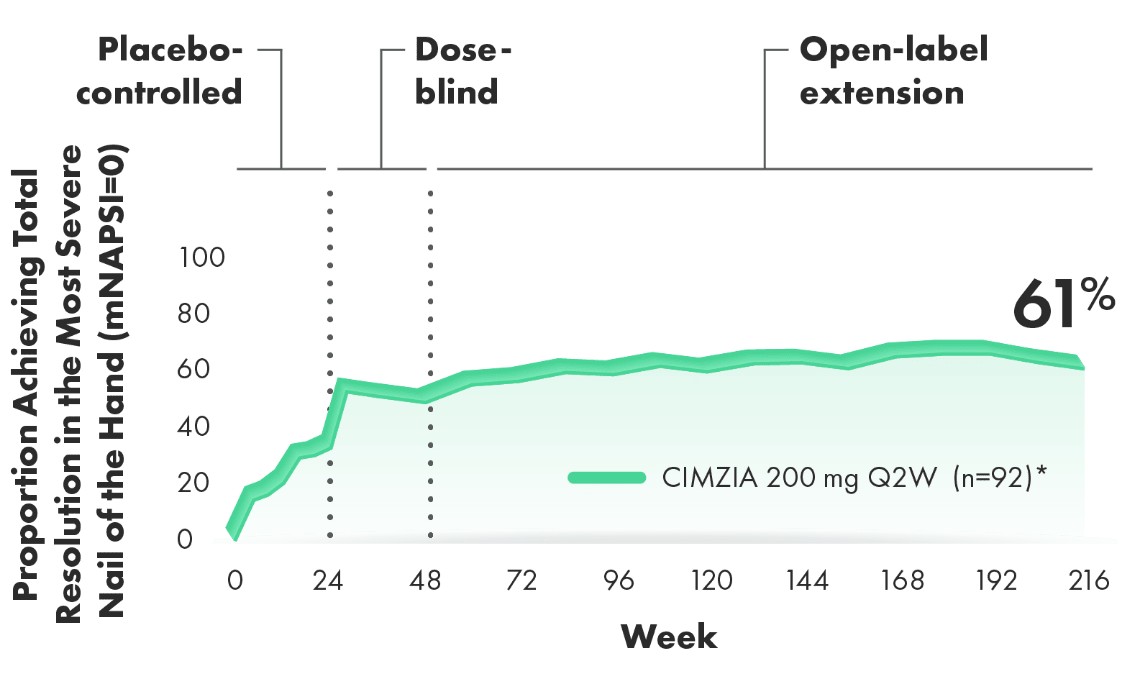
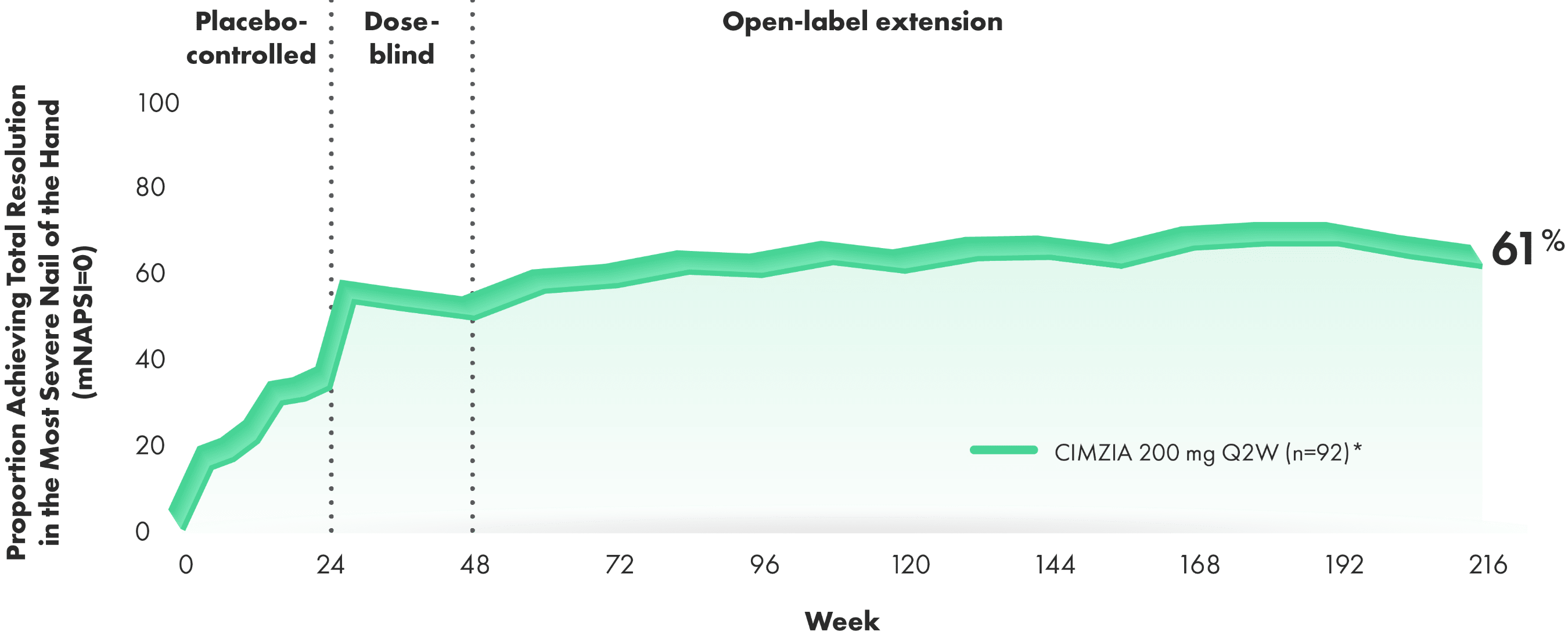
~6 OF EVERY 10 PATIENTS WITH BASELINE INVOLVEMENT ACHIEVED TOTAL RESOLUTION OF NAIL PSORIASIS OVER 4 YEARS3,4
Post hoc analysis: Total resolution rates for nail psoriasis in the most severe nail of the hand are presented for patients affected by this condition at baseline. This condition was defined at baseline as mNAPSI >0 for nail psoriasis.3,4
- Change from baseline in mNAPSI score in the subgroup of subjects with psoriatic nail disease at baseline was a prespecified other efficacy variable
- Limitations of OLE data include potential for enrichment of long-term data in the remaining patient population, as those who remain in the study generally fare better than those who discontinue. This subgroup analysis is a post hoc analysis. The RAPID-PsA study was not powered for this subgroup analysis, nor was the analysis error controlled. Therefore, these results should be interpreted with caution, and the data observed in this subgroup cannot be regarded as statistically significant
*92 patients of the 138 patients in the CIMZIA 200 mg Q2W arm had baseline nail disease and were evaluated through Week 216.
RAPID-PsA2
RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and open-label through Week 216. In this study, 409 patients who had failed ≥1 DMARD (non-biologic or biologic) were randomized (1:1:1) to CIMZIA 200 mg Q2W (n=138), CIMZIA 400 mg Q4W (n=135), or placebo (n=136). Patients were stratified by prior TNFi exposure; primary nonresponders were excluded.
CZP, certolizumab pegol; DMARD, disease-modifying antirheumatic drug; LDI, Leeds Dactylitis Index; LEI, Leeds Enthesitis Index; LOCF, last observation carried forward; mNAPSI, modified Nail Psoriasis Severity Index; OLE, open-label extension; PsA, psoriatic arthritis; Q2W, every 2 weeks; Q4W, every 4 weeks; RS, randomized set; TNFi, tumor necrosis factor inhibitor.
Improvement in signs and symptoms regardless of prior TNFi experience3,4
ACR20/50/70 response at Year 43*
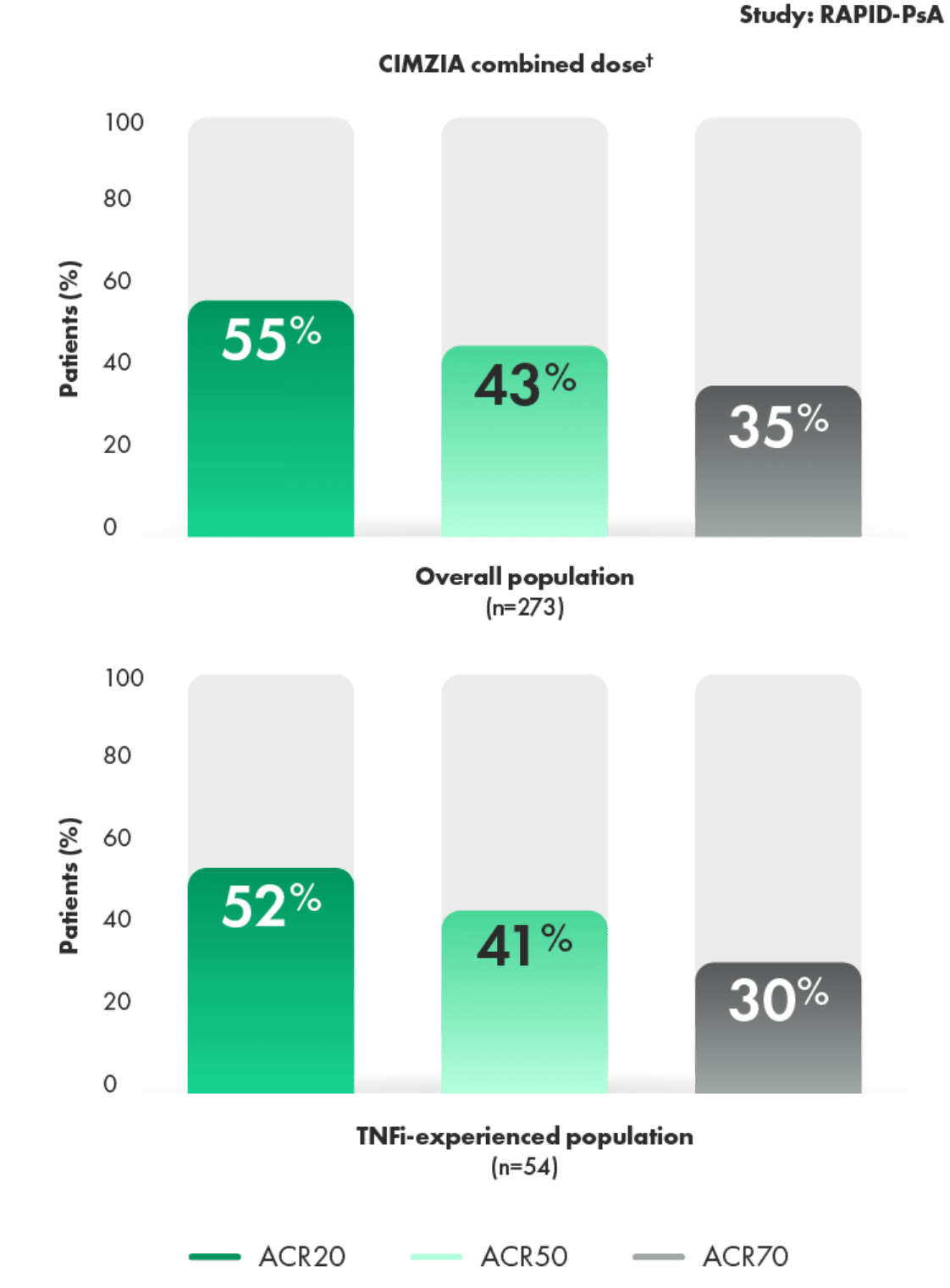
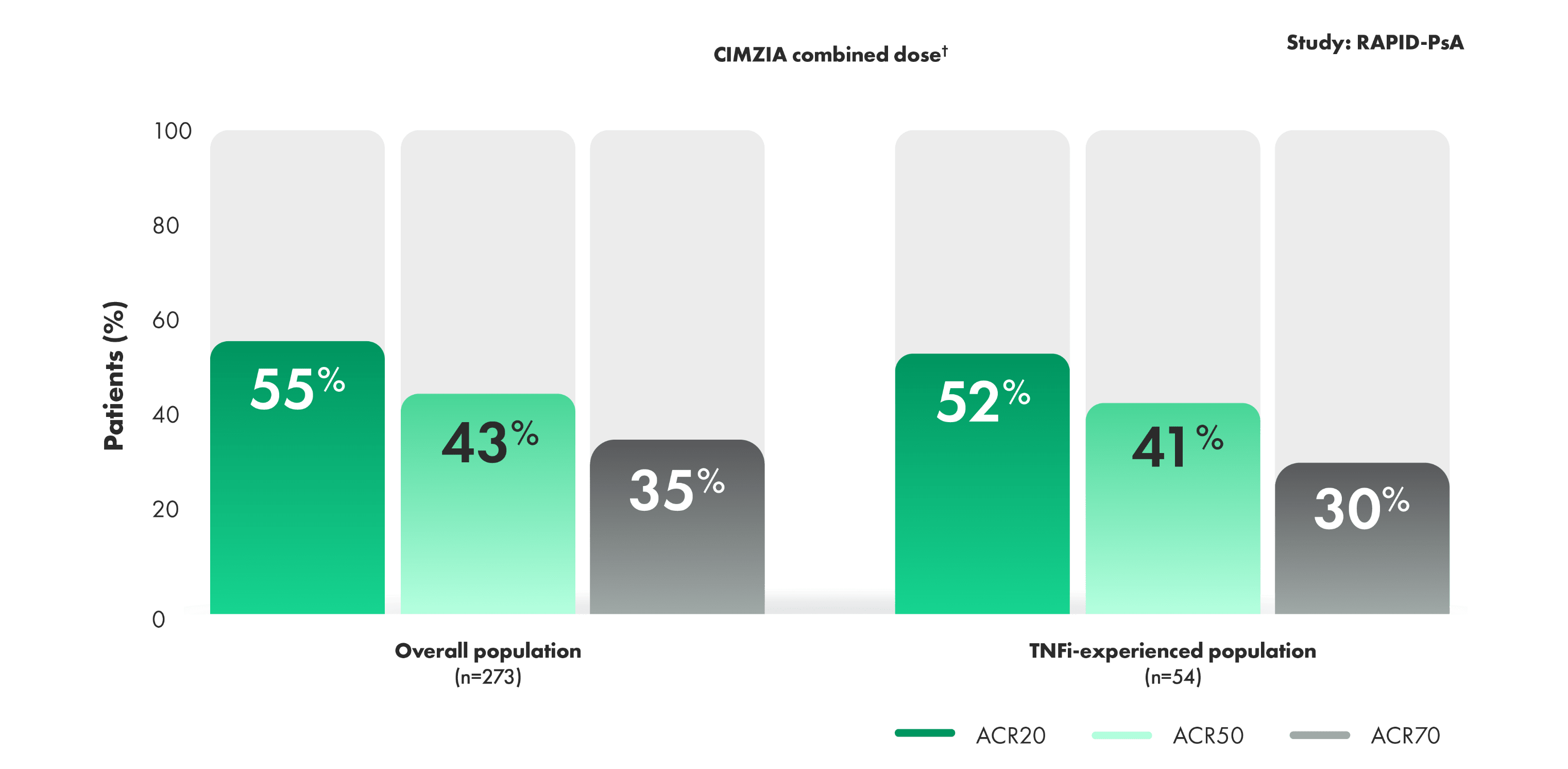
- Primary efficacy variable of ACR20 response at Week 12 (P<0.001). ACR20 responses for CIMZIA 200 mg Q2W and placebo were 58% and 24%, respectively1,4
- 20% of patients had prior TNFi exposure, primary nonresponders excluded1,4
- Limitations of OLE data include potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
*RS-NRI: randomized set nonresponder imputation.
†CIMZIA combined dose included patients receiving CIMZIA 200 mg Q2W and patients receiving CIMZIA 400 mg Q4W.
RAPID-PsA2
RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and open-label through Week 216. In this study, 409 patients who had failed ≥1 DMARD (non-biologic or biologic) were randomized (1:1:1) to CIMZIA 200 mg Q2W (n=138), CIMZIA 400 mg Q4W (n=135), or placebo (n=136). Patients were stratified by prior TNFi exposure; primary nonresponders were excluded.
ACR, American College of Rheumatology; DMARD, disease-modifying antirheumatic drug; OLE, open-label extension; PsA, psoriatic arthritis; Q2W, every 2 weeks; Q4W, every 4 weeks; TNFi, tumor necrosis factor inhibitor.
MDA: A holistic treatment goal for patients with PsA
MDA is a single holistic treatment goal that encompasses multiple measures commonly used by rheumatologists to assess PsA patients.






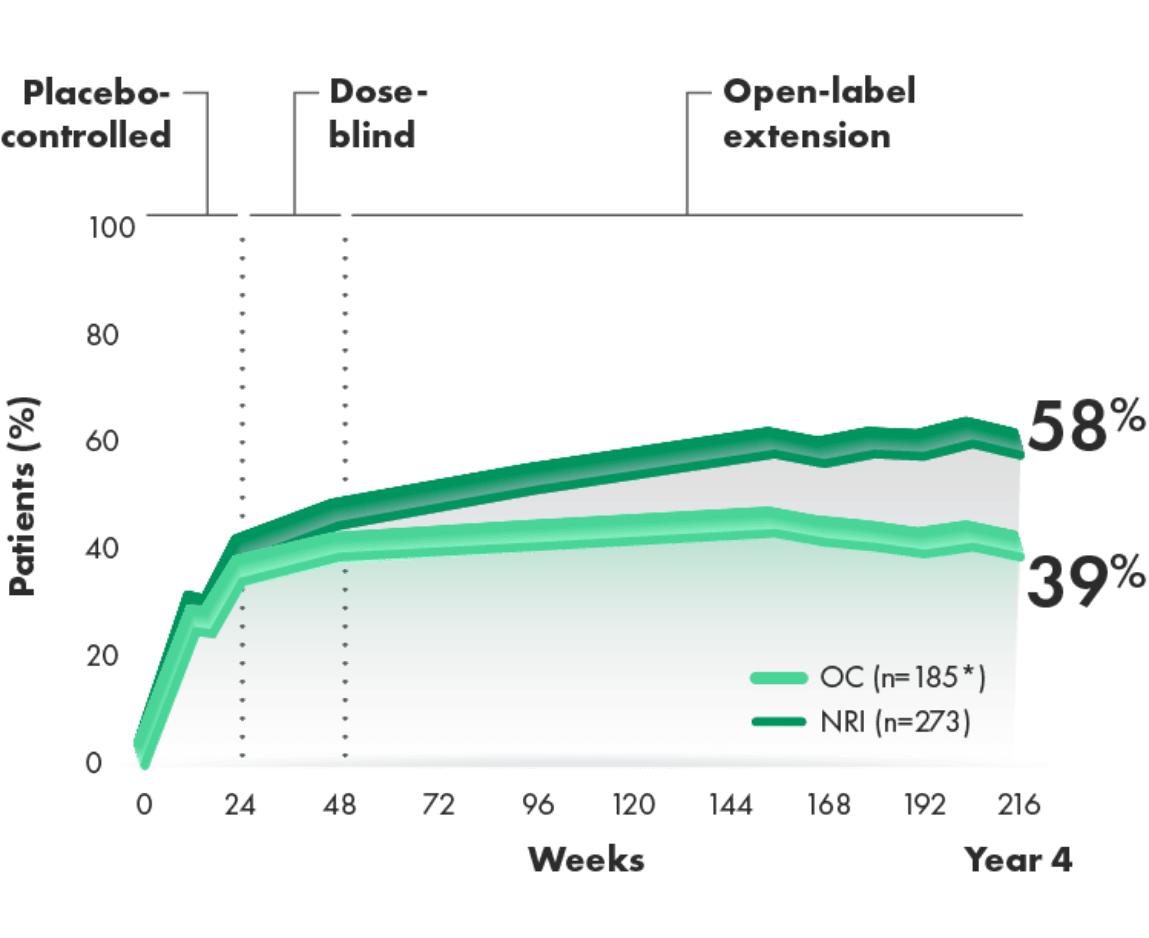
CIMZIA helped ~6 of 10 patients achieve MDA at Year 43
MDA over 216 weeks (post hoc analysis of combined doses from 4-year OLE of RAPID-PsA)3
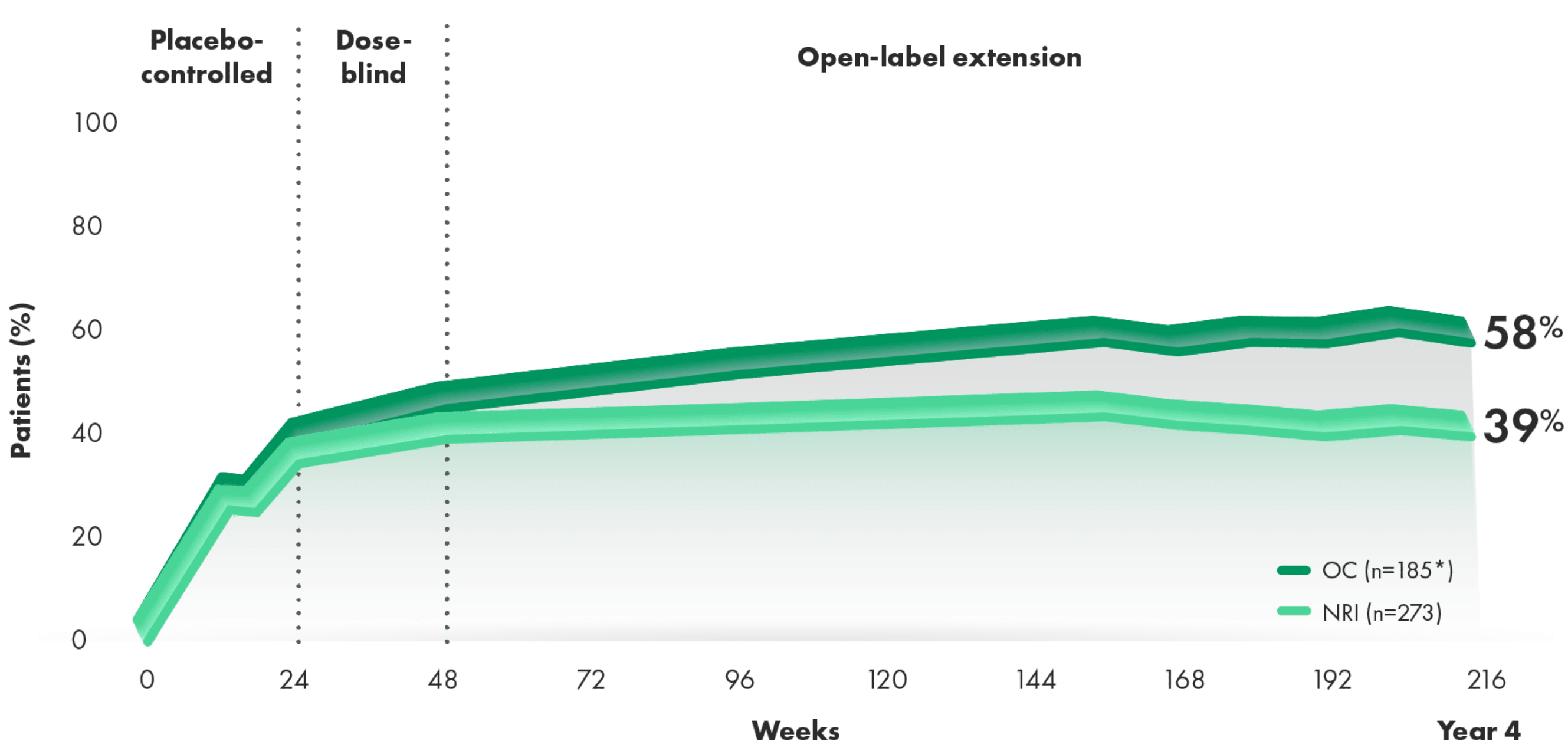
STUDY POPULATION INCLUDED BIO-NAÏVE AND BIO-EXPERIENCED PATIENTS
Post hoc analysis: In RAPID-PsA, MDA (fulfilling ≥5 of 7 criteria) in patients randomized initially to either CIMZIA dose level (200 mg Q2W or 400 mg Q4W) was analyzed post hoc.
At Year 4:
- 58% and 39% of CIMZIA-treated patients achieved MDA by OC and NRI, respectively
- Limitation of OLE: Responder rates do not have long-term placebo comparator beyond Week 24
*n at Week 216.
GRAPPA: Updated treatment recommendations for PsA 20216
In the most recent update to GRAPPA treatment recommendations, the goals of therapy for all patients with PsA are:
- To achieve the lowest possible level of disease activity, including LDA or MDA in all domains of disease
- To optimize functional status
- To minimize complications
See guidelines for full recommendations. This information is not intended to be medical advice.
RAPID-PsA2
RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and open-label through Week 216. In this study, 409 patients who had failed ≥1 DMARD (non-biologic or biologic) were randomized (1:1:1) to CIMZIA 200 mg Q2W (n=138), CIMZIA 400 mg Q4W (n=135), or placebo (n=136). Patients were stratified by prior TNFi exposure; primary nonresponders were excluded.
DMARD, disease-modifying antirheumatic drug; GRAPPA, Group for Research and Assessment of Psoriasis and Psoriatic Arthritis; LDA, low disease activity; MDA, minimal disease activity; NRI, nonresponder imputation; OC, observed case; OLE, open-label extension; PsA, psoriatic arthritis; Q2W, every 2 weeks; Q4W, every 4 weeks; TNFi, tumor necrosis factor inhibitor; VAS, visual analog scale.
CIMZIA helped patients achieve a reduction in pain that lasts
Change from baseline in patient global assessment of arthritis pain through
Year 43,4*† Change from baseline in patient global assessment of arthritis pain through Year 43,4*†
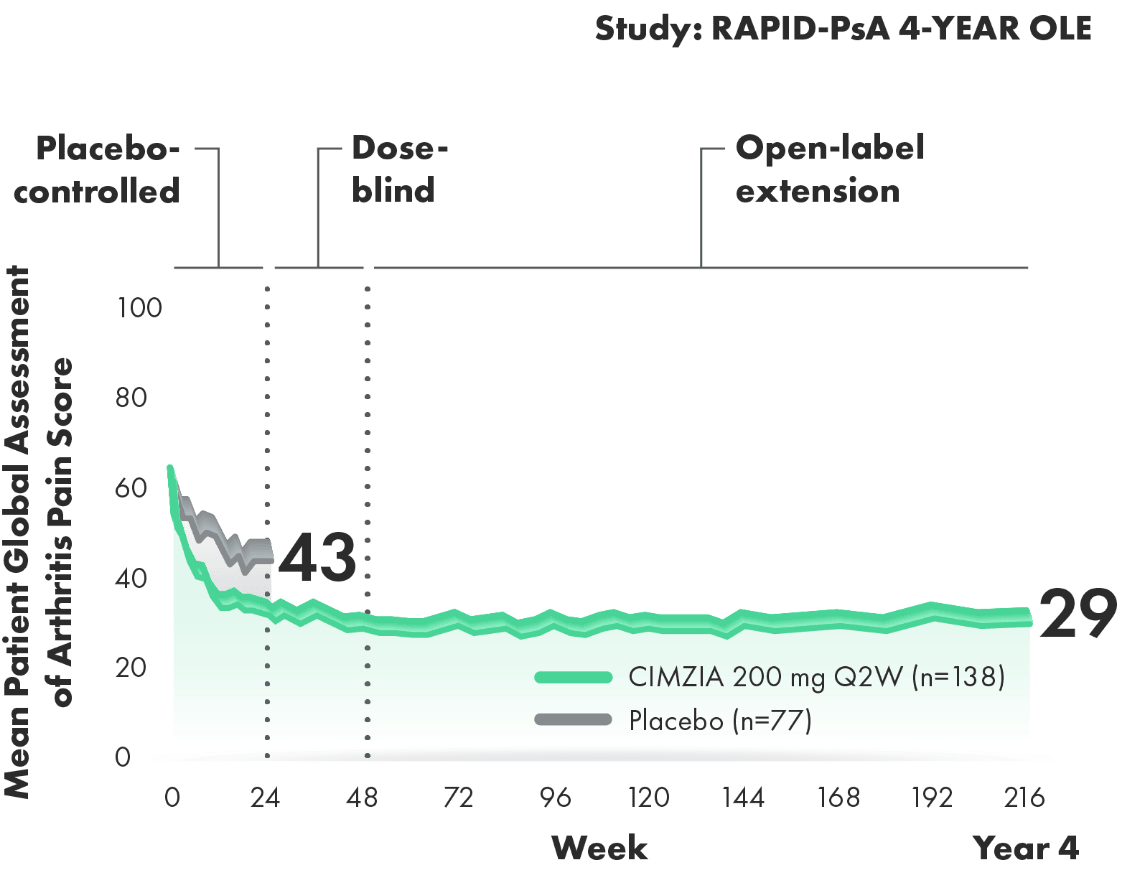
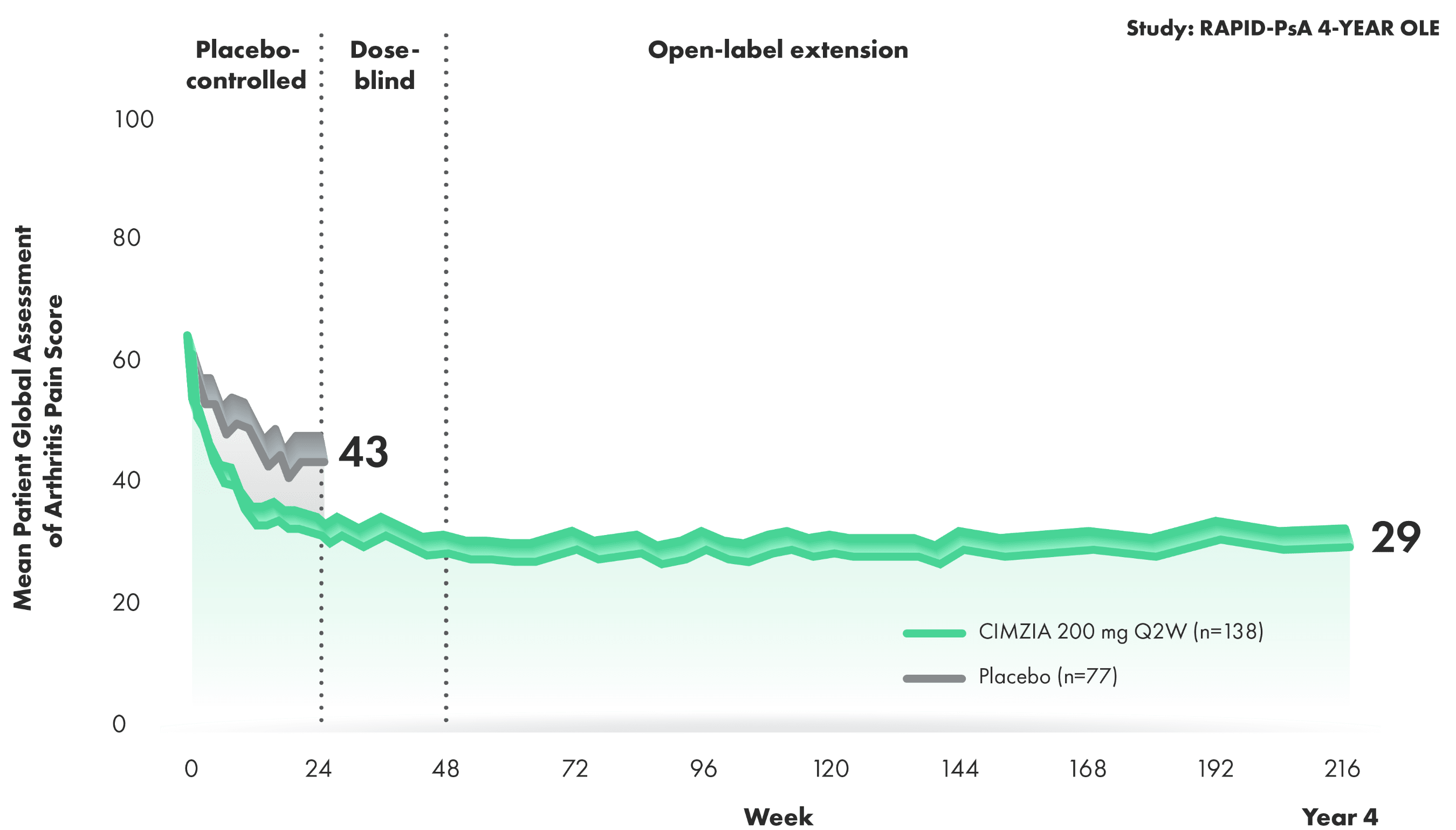
50% REDUCTION IN PAIN SCORE AT YEAR 4 WITH CIMZIA 200 mg Q2W3,4
- Baseline pain score was 60 (VAS: 0=no pain and 100=most severe pain) for both the placebo arm and the CIMZIA 200 mg Q2W arm3,4†
- Limitations of OLE data include potential bias due to open-label treatment and lack of long-term placebo control beyond Week 24
*Pain assessment is a part of the ACR score. Pain assessment is done by the patient, hence individual assessment/score may vary from patient to patient. Patient assessment of arthritis pain, VAS: 0=no pain and 100=most severe pain.
†Randomized set. LOCF is used for missing data, early withdrawals, or placebo escape.
RAPID-PsA2
RAPID-PsA was a randomized, multicenter, Phase 3 trial in patients with active PsA. The trial was double-blind and placebo-controlled through Week 24, followed by an extension study that was dose-blind through Week 48 and open-label through Week 216. In this study, 409 patients who had failed ≥1 DMARD (non-biologic or biologic) were randomized (1:1:1) to CIMZIA 200 mg Q2W (n=138), CIMZIA 400 mg Q4W (n=135), or placebo (n=136). Patients were stratified by prior TNFi exposure; primary nonresponders were excluded.
Help improve 8 key functions in patients’ daily lives
Mean improvement from baseline in physical function—PsA HAQ-DI improvement through Week 241,2,4‡
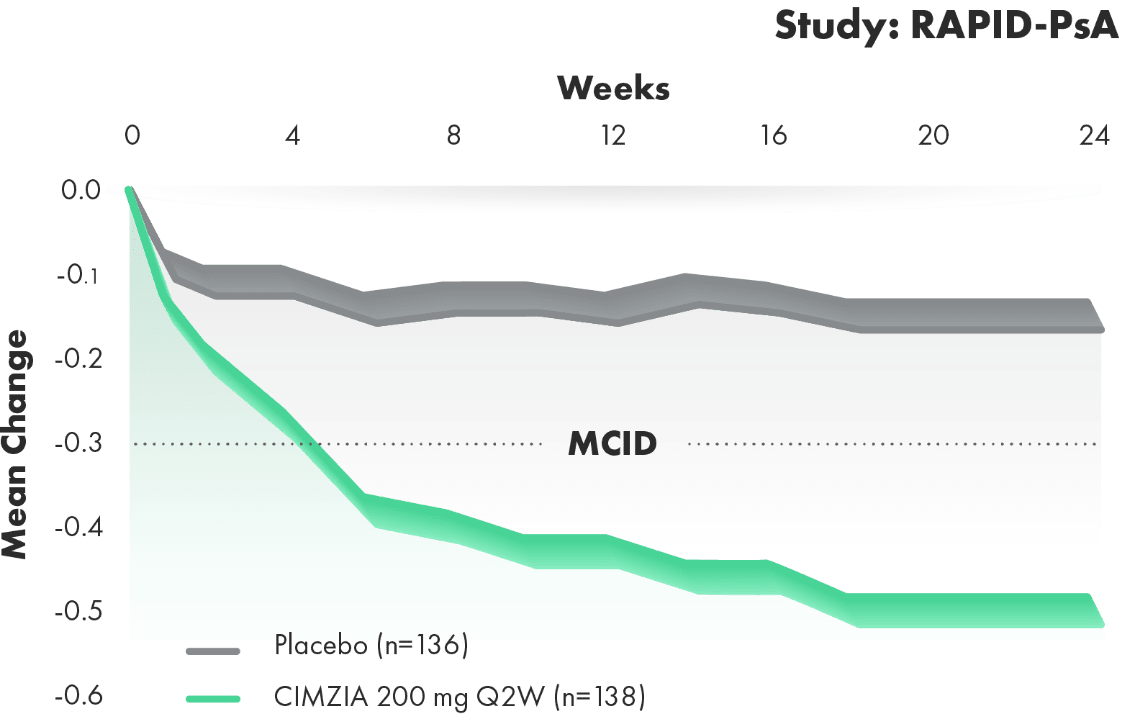
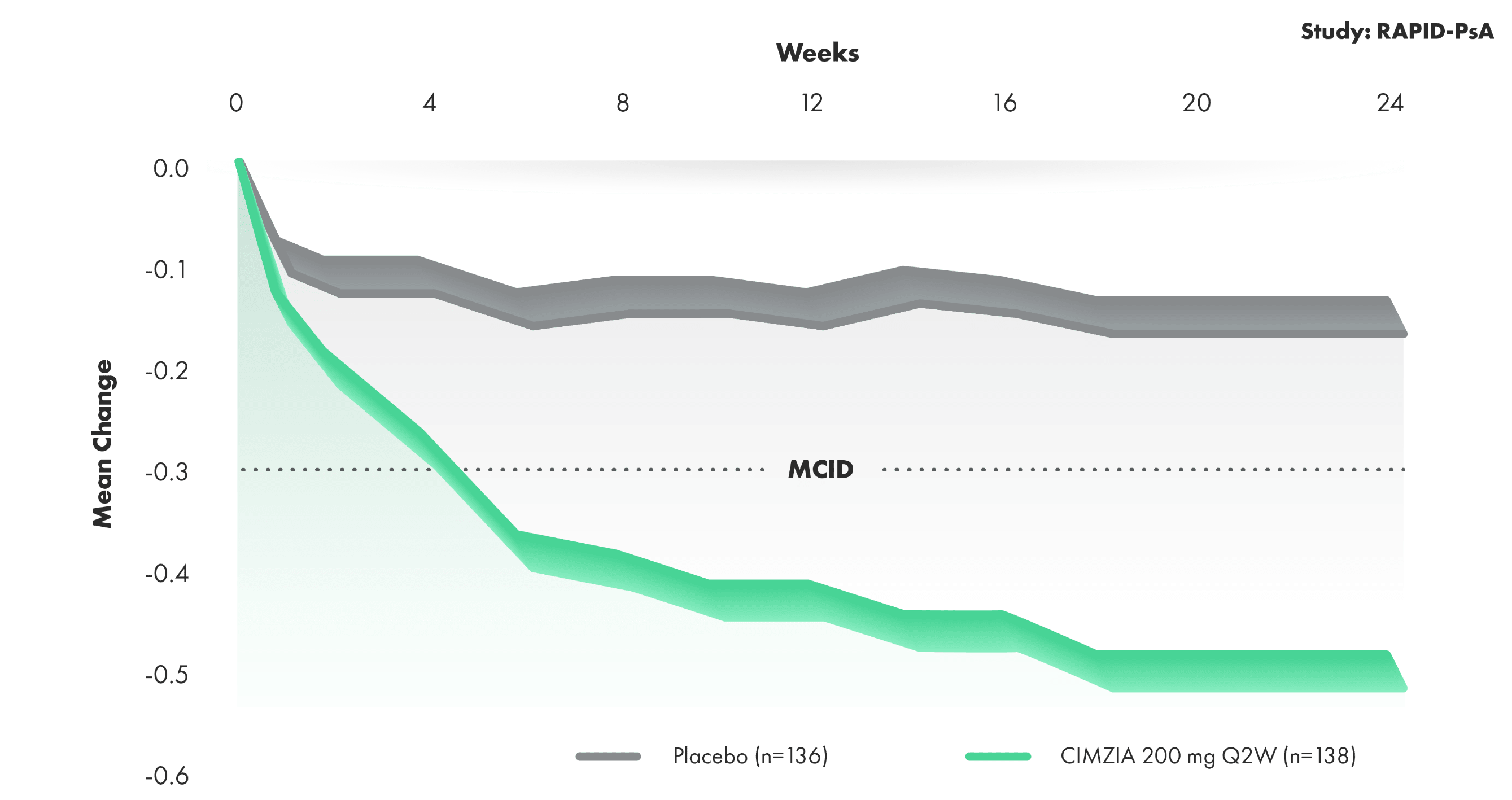
8 meaningful measures for patients: HAQ-DI
- Change from baseline in HAQ-DI scores represents improvements in patients’ ability to perform certain activities of daily living in the RAPID-PsA study. Physical function was a prespecified end point
- MCID was defined as a reduction in HAQ-DI from baseline of ≥0.3
‡ITT-LOCF: intent-to-treat last observation carried forward.
ACR, American College of Rheumatology; DMARD, disease-modifying antirheumatic drug; HAQ-DI, Health Assessment Questionnaire Disability Index; LOCF, last observation carried forward; MCID, minimum clinically important difference; OLE, open-label extension; PsA, psoriatic arthritis; Q2W, every 2 weeks; Q4W, every 4 weeks; TNFi, tumor necrosis factor inhibitor; VAS, visual analog scale.
Safety profile through 24 weeks in RAPID-PsA1,2
Incidence of TEAEs through Week 242
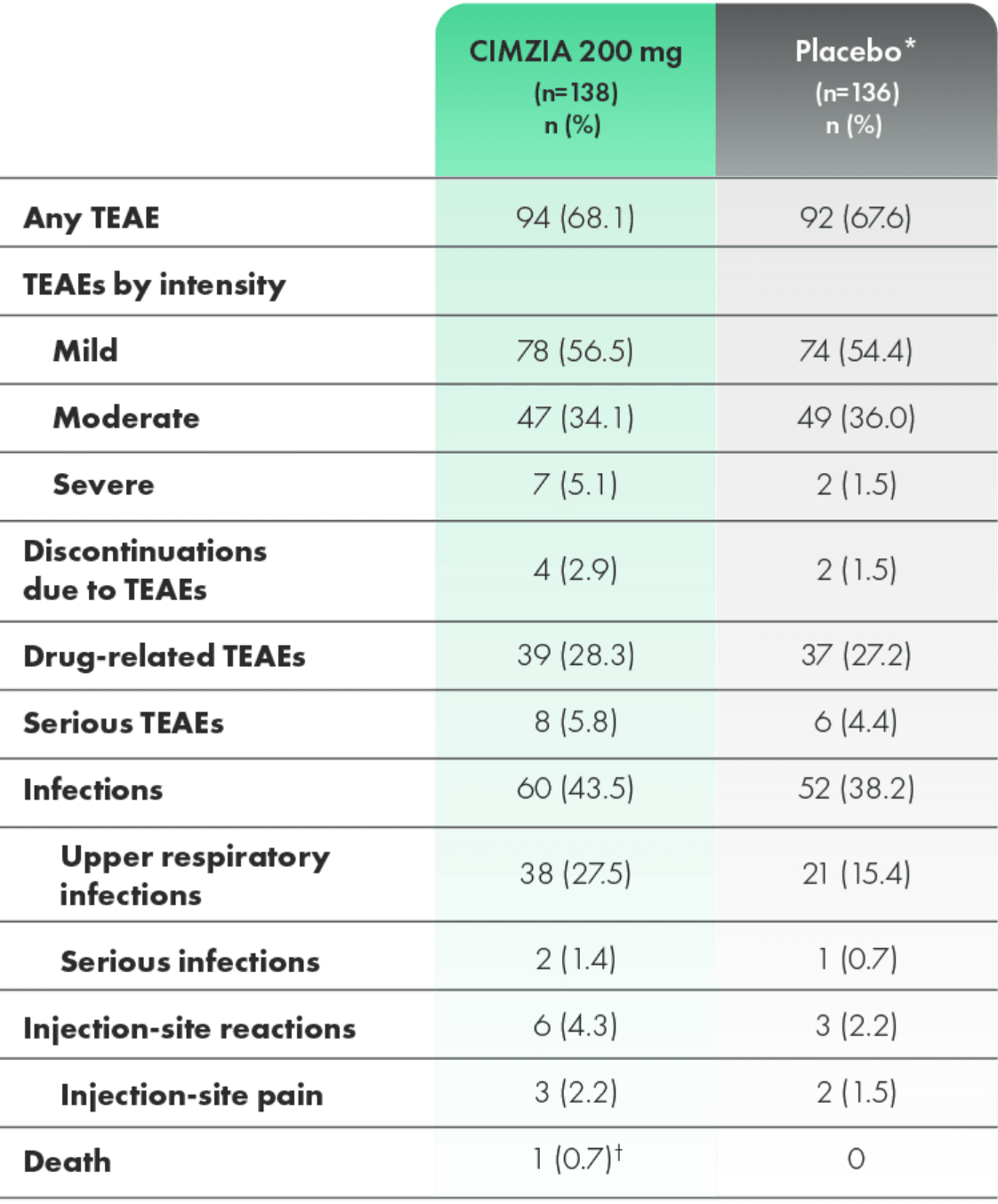
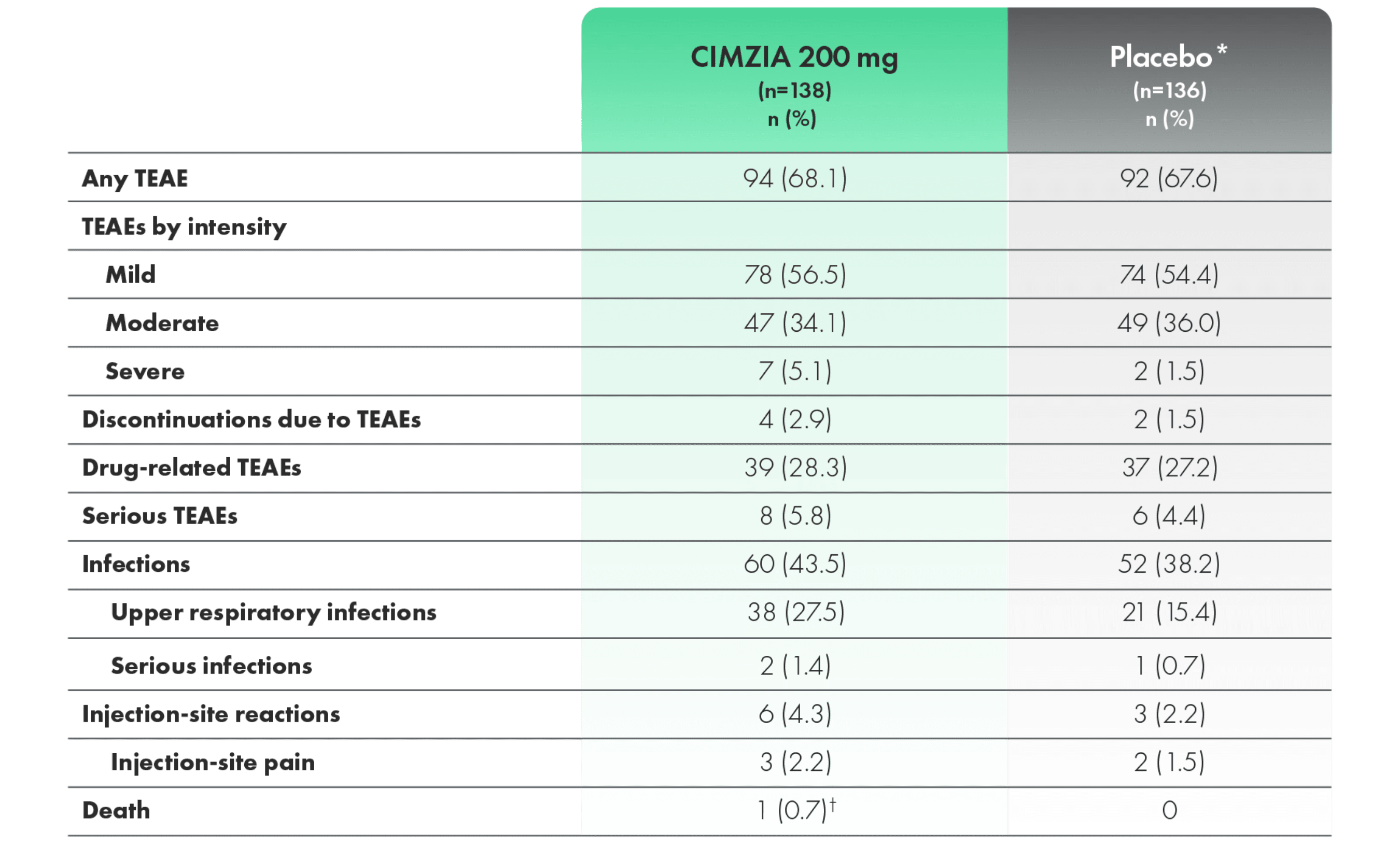
*Placebo escape at Week 16; data not adjusted for exposure.2
†Myocardial infarction. Considered unrelated to study medication by investigators.2
TEAEs with an incidence of >3% of patients (CIMZIA 200 mg) through Week 241,4
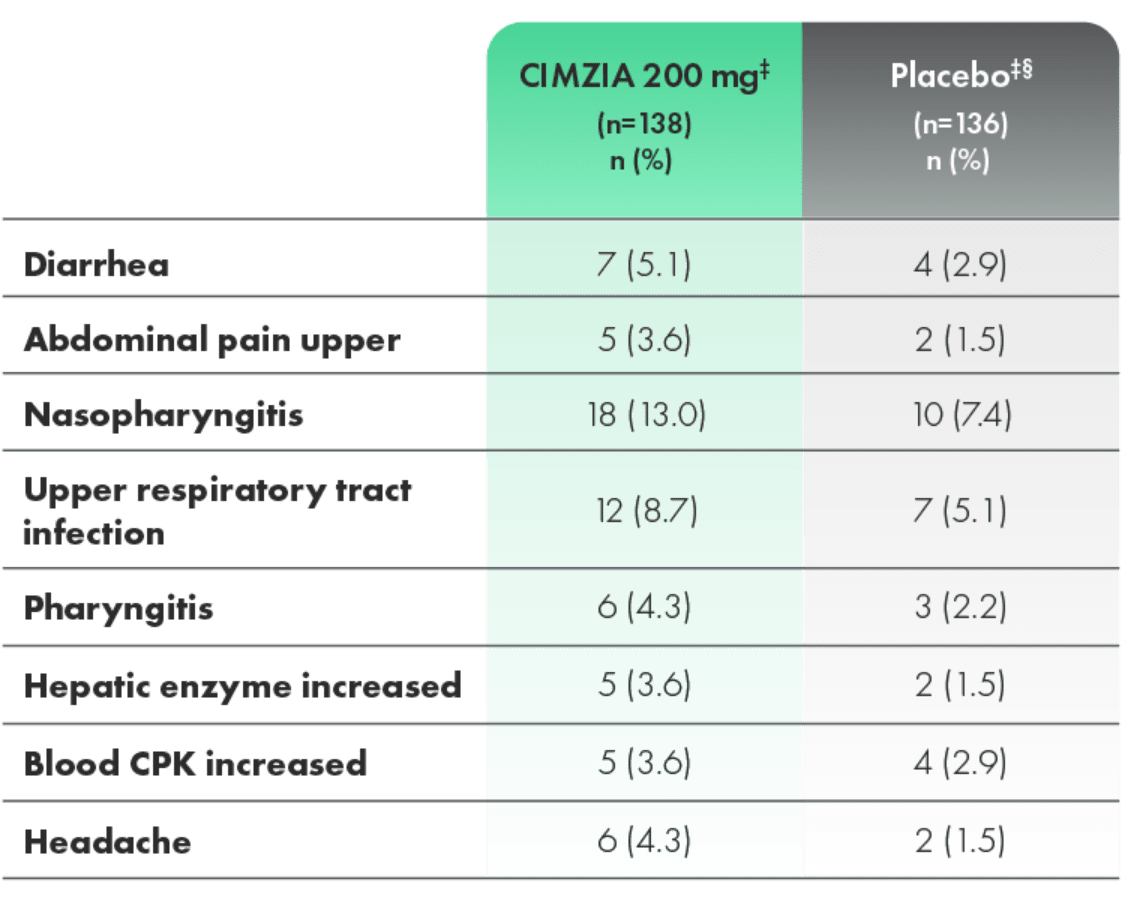
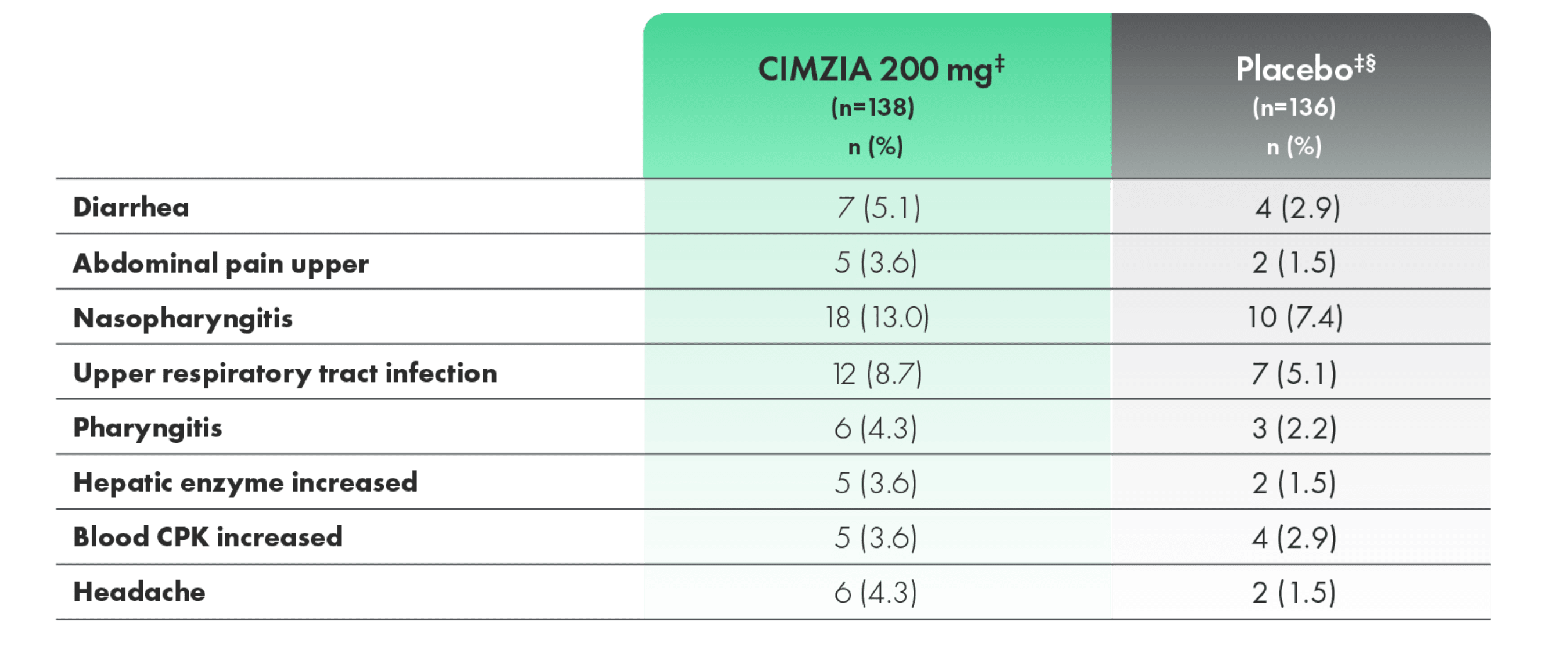
- Most adverse events were mild to moderate in severity
‡Not adjusted for exposure.
§Placebo escape at Week 16.2
CPK, creatine phosphokinase; PsA, psoriatic arthritis; TEAE, treatment-emergent adverse event.
Fc, fragment crystallizable; PEG, polyethylene glycol; TNF, tumor necrosis factor.